Vaccine Q&A, 19Feb2021
Georgia COVID-19 Updates

Happy Friday! This is the second edition of Vaccine Q&A for this newsletter. You can read last week’s edition here. Before we get going, I just want to remind my readers that I am not a medical doctor and cannot provide medical advice. Always consult your physician for addressing your unique medical needs. This newsletter is instead more of a general understanding of the science and an attempt to provide clarity on some of the pressing questions that people have about the vaccine. Overall, the vaccines have been shown to be safe and effective, nearly eliminating the risk of severe infection that results in hospitalization and/or death. But I think it’s fair to ask questions and desire answers. My ultimate goal is to answer your questions to the best extent possible with data so that you feel empowered and informed about your decision, either way.
I’ve written on this topic previously, so I’ll refer you to some links below that may answer some of the “how” questions.”
How the immune system works (a simplified crash course)
A crash course on cell and molecular biology and how the RNA vaccines work
Efficacy data for the Pfizer and Moderna vaccines
The DNA vaccines from Johnson and Johnson and AstraZeneca, also a discussion of how we anticipate the vaccines will do against the variants and some information on vaccine trials taking place for children.
Comparing the efficacy of the RNA vaccines versus the Johnson and Johnson vaccine
I received my first dose of the Moderna vaccine on Wednesday. I’ll let you know that I’ve had a sore arm since the injection, but nothing that required pain medication. I also had insomnia the first night but I have been working under a deadline lately and I suspect that had to do with it more than the vaccine. Either way, I reported it to v-safe, the CDC’s safety tracking app.
Today we’re going to talk a lot about vaccine logistics.
Why do I need two doses?
Refer back to this newsletter where I discussed the efficacy data from the clinical trials for Moderna and Pfizer. The short answer is yes, you need two doses. Getting just one dose provided 52% efficacy. It wasn’t until the second dose that >90% efficacy was achieved. If you have already received one dose of the vaccine, please make sure to get the second dose. Not only would you not be protected to the same extent as a 2-dose recipient, but with resources as limited as they are you’ve potentially taken a dose away from someone who would complete the 2-dose series. Please get the second dose done.
When the Johnson and Johnson vaccine receives Emergency Use Authorization (EUA), then it will just be a single dose.
When do I get my second dose?
So far there are two vaccines available for use in the US, from Pfizer and Moderna, each of which are a two-dose series. For Pfizer, the interval between doses is 3 weeks. For Moderna the interval if 4 weeks.
It’s a good idea to schedule your second dose as soon as you get your first one, since supplies are limited and so are appointments. What happens if you miss the time interval? As in, 3-4 weeks later you haven’t gotten your shot. We don’t have guidance from CDC or the vaccine manufacturers on a maximum delay after which a person would need to repeat the series. Instead, the Advisory Committee on Immunization Practices just says to get the second dose as soon as possible. Looking at the Pfizer administration guide, they indicate trying to do so within 6 weeks of the first dose. For me, getting the vaccine on Wednesday means that I’m due for the second dose during the middle of Spring Break for my kids. Guess who isn’t going anywhere for Spring Break? This vaccine is that important to me. We will “staycation” and sightsee from a safe social distance in our local area.
The United Kingdom has prioritized getting as many people their first dose of the vaccine as possible, even at the expense of getting people their second dose. As a result their dosing interval has been extended. We’ll have to see how well that works for them, but the clinical trial data indicated the optimal interval was 3 weeks for Pfizer and 4 weeks for Moderna. We should be making evidence-based decisions. Perhaps we will learn from the UK that 6+ weeks between doses still seems to work. But in this country, our regulatory bodies don’t make policy decisions based on opinion or suggestion. I think it would harm public trust to do things that way. Instead, FDA requires controlled studies and large sample sizes.
Can we mix and match vaccine manufacturers for dose 2?
No, it’s best to stick with the same vaccine manufacturer as you had during the first dose. We do not have data to know whether switching will result in protection and we don’t have safety data for doing so either.
Storage conditions
This one came from my father-in-law, a retired veterinarian: the vaccines are stored in ultracold freezers, does that mean I’ll feel really cold when the vaccine is given to me? Short answer is no, for at least two reasons: (1) they thaw the vaccine and then mix it with a liquid (this is Pfizer specific, no mixing for Moderna) before they’re administered, and (2) the volume of liquid injected is small enough that you likely wouldn’t sense a temperature difference anyway.
The Pfizer vaccine is the one that requires ultracold storage (-80C). These types of freezers are most common at laboratories, hospitals, universities, etc. The Moderna vaccine is stored in a -20C freezer, similar to the freezer you have as part of your kitchen refrigerator. This might mean that more rural counties or areas with fewer healthcare centers have more of the Moderna vaccines than Pfizer ones.
Once the vaccines are thawed and the vials are punctured, they need to be used within 6 hours. After that, they are to be thrown away. That’s how I managed to get my vaccine. I got a “leftover” dose at the end of a scheduled vaccine clinic. That’s also the reason why the state has focused on appointment-based vaccine deployment - to make sure they are thawing just enough doses. The doses are ineffective after that time because of how unstable the RNA in them can be. One reader asked if it would be harmful to be vaccinated after the 6 hour window. I don’t think it would be unsafe but it likely wouldn’t work. And I would hate for you to have a false sense of security. That’s why the healthcare workers at the vaccine clinics are keeping a careful eye on the time.
As of a recent report, Georgia has thrown away 3,887 doses, and about half were because they couldn’t find someone to give the vaccine to (“not needed after prep”). It’s a shame that any doses are going in the trash. But it’s good to know that the number isn’t larger than this.


However, the Governor announced yesterday that GEMA and the Georgia National Guard are setting up mass vaccination clinics at four locations: the Atlanta airport, Macon-Bibb county, Albany, and the Habersham County Fairgrounds in Clarkesville. But you need to pre-register to participate. Pre-registration will also help them to determine how many people are coming and thaw only what is needed. I encourage you to take advantage of these options, even if they are not in your immediate area. My husband’s parents took advantage of a mass vaccine clinic in Missouri. From their experience, I will suggest that you take snacks and a book and be ready to sit in your car for a while, just in case. I think the vaccine is worthy of the hassle.
What are the vaccine ingredients?
For Pfizer, you can read the FDA document here and the ingredients are found on page 2.

And for the Moderna vaccine, see page 2 also.

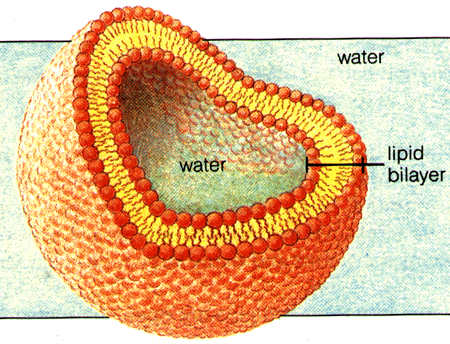
mRNA is the most important part of this vaccine - it is a nucleic acid (a kind of biomolecule) that codes for the spike protein that is normally made by the SARS-CoV-2 virus. Lipids are another class of biomolecule that include fats and oils. A special kind is called a phospholipid and these molecules sandwich together to form the membranes of your cells. Some viruses have an envelope, which is analogous to our cell membrane. In fact, they sort of steal membrane from our cells before they break lose to infect neighboring cells. The lipids described here in the ingredient list are like these phospholipids that your cells produce naturally. What’s pretty cool about these phospholipids is one end of the molecule repels water (look like tails in the graphic below) and one end is attracted to water (look like balls in the graphic below), so they naturally form this dual-layered membrane where the water-avoiding ends are held together on the inside (yellow areas in the graphic) and the part that likes water is facing the outside (red balls). The end result is we get this bubble with water in the middle, called a liposome. The mRNA for the vaccines is held in the interior space where the graphic below says “water.” This liposome is just a delivery vehicle, keeping the mRNA safe until it gets to your cells.
The other things in the ingredient lists are mostly ions (think electrolytes) that help keep the liposome stable. Your cells are not filled with pure water, they have positively and negatively charged ions in them. And if we put your cells in pure water they would explode because of osmosis (probably lots of mental cobwebs here). Essentially, the pure water on the outside of your cells would rush into your cells to try to equalize the ion concentration both inside and outside of the cell. Ions are also needed to help biomolecules (i.e. carbohydrates, proteins, lipids and nucleic acids (DNA/RNA)) hold their shape. For these reason, we virtually never store biological molecules in pure water. And when you’re dehydrated, you’re not given pure water in an IV bag at the hospital - it always has saline (salt solution) and sometimes sugar. When you see sucrose in the ingredient list for the vaccines, that’s table sugar. Tromethamine is a buffer - used to keep solutions at a stable pH (like Goldilocks, not too acidic, not too basic). Having the wrong pH can change the shape of biomolecules like the phospholipids or the mRNA, making them less stable.
Do these vaccines contain microchips? From the ingredient list, we can see that they’re not present. I think this is a rumor aimed at disinformation and I’m sorry that someone shared it with you. This is someone taking advantage of your fear and anxiety. There are no microchips. If you have genuine fear about someone tracking your whereabouts, then it’s probably time to get rid of your smartphone, smartwatch and digital footprint. Because you willingly share far more than you might realize.
Should I get the vaccine if I’ve already had COVID-19?
Yes. But if you would prefer to wait until vaccine supply is more plentiful, I think that’s fine to do. We don’t know how long immunity lasts after infection so I think, to be safe, we want to give everyone the same baseline of immunity as best as we can. However, we know immunity lasts at least 90 days and possibly longer after infection. So if you want to wait and give someone else the vaccine, I think that’s probably fine and certainly admirable.
If you were treated with monoclonal antibodies during your infection with COVID-19 then the guidance is to wait at least 90 days until after that treatment before getting the vaccine. This is an infusion via IV line so you would know it if you received this therapy. But you can check with your physician also if your case required a hospital stay. The reason being is that during this treatment your body was flooded with antibodies (not your own) to bind up as many viral particles as possible before they could attach to your cells. This is called passive immunity - where you don’t generate an immune response but take advantage of someone else’s. A more familiar example is antibodies transmitted from mother to baby through breastmilk. Antibodies can last as long as 90 days. So the 90 day waiting period is to allow your body to clear out the artificial and passive immunity that you got from the monoclonal antibodies so that your immune system is what makes the antibodies when the vaccine is administered.
If you were not treated with monoclonal antibodies, then the guidance is to wait until you’ve completed the isolation period that goes with your infection. That isolation period is 10 days since your symptoms began AND 24 hours fever-free AND if your other symptoms are improving. The purpose of this is to prevent you from accidentally giving the virus to the healthcare workers and other vaccine recipients at your appointment. You do NOT have to wait 90 days after the infection to get the vaccine. However, it is completely fine to wait that long if you want to defer to others.
Should I get the vaccine if I’m exposed or sick in between doses?
This actually happened to my brother-in-law’s mother. She got exposed through her granddaughter’s daycare. Okay, so you’ve had dose one, but some time during that 3-4 week span afterwards you’ve either had a high risk exposure or maybe you’ve gotten sick.
If it was an exposure, then follow the quarantine guidelines from CDC (safest to do so for 14 days). We don’t want you to get people sick at the vaccine appointment. The good news, is there is some grace period on getting the second dose (6 weeks, according to the Pfizer administration guide referenced in the above sections). We just need to adjust. So, ideally, wait 14 days and then go get dose #2.
If you get sick, then you follow the isolation guidance described in the section just above this one. When your 10 days are complete, then you can get the second dose provided it’s the right time in your dosing schedule.
Once you’ve received both doses of the vaccine, continue to be careful for at least 10-14 days after the second dose. We want you to complete your immune response after the second dose. After that time, you do NOT have to quarantine if you are exposed to someone with COVID-19. This is true for at least 90 days afterwards and possibly/very likely longer. It’s unclear how long the immunity from the vaccine will last, just as we don’t know for natural infection. But we know for sure that it lasts at least 90 days. I would not be surprised if this guidance extends to a longer length of protection as more data are collected to confirm long lasting immunity. The Emergency Use Authorization is not the same thing as FDA approval. It is a go ahead for use but they want continuing data collection and submission for review to achieve full FDA approval. Pfizer and Moderna are continuing to collect data from their clinical trials, including checking to see how long their participants remain disease-free after receiving the vaccine. They gain more data with each passing day. So make sure your knee-jerk reaction to the CDC guidance on post-vaccination exposure isn’t to say that vaccines only provide immunity for 90 days. This guidance, and particularly that statement from CDC, is a cover-your-butt sort of liability statement because we just don’t have enough data yet.
Reactogenicity and NSAIDs
There are known side effects associated with the vaccines that are the result of having an immune response. Reactogenicity means the ability to generate a reaction and it pertains to these vaccines. The cardinal signs of inflammation that every nurse and doctor are taught are redness, swelling, heat and pain (and sometimes loss of function). Inflammation is part of your immune response, even when not directly due to an infection. Meaning, if you have a splinter or a sunburn or an infection like an abscess in your skin, you will notice that the area will be red, be swollen or raised, it might hurt so much that you avoid using that part of your body and it will be warm to the touch. If the inflammation is localized, like a splinter, then only a small part of the body is impacted. If you have an infection that affects multiple areas of your body (like influenza or COVID-19), you might have more body-wide (systemic) effects like a fever, fatigue, headache, etc. These are expected to happen and a sign that your immune system is reacting to something and mounting a response against it. If you don’t have these symptoms that does not necessarily mean that you didn’t mount an immune response. You’re probably just lucky. The table below shows the symptoms you might expect after receiving each of the vaccines. Things you’ll notice are that the numbers are slightly higher for Moderna than Pfizer for dose 1 and dose 2 is higher than dose 1. But they aren’t drastically higher to the point that I would consider one vaccine manufacturer superior to the other. I would take whichever vaccine is offered to you first.

Myalgia may be a new word for some of you. It means muscle pain or aching. I will say for my experience getting 1 dose of the Moderna vaccine, I only had two of these symptoms - pain at the injection site and fatigue. That makes sense since they’re two of the most common. My husband had pain, fatigue, headache and myalgia. I did not require pain medication. My husband did take pain medication. And I would do it again - a day or two of a sore arm is far better than being sick with something that could land me in a hospital bed, on a ventilator, etc.
To recap, the symptoms outlined in the graphic above are NORMAL and EXPECTED. When you get your vaccine, you’ll get a piece of paper that invites you to report your symptoms to the CDC via v-safe. This is one of three COVID-19 vaccine safety programs ongoing right now that will feed into a larger analysis of the vaccine’s safety. PLEASE consider helping out with this effort, even if you’re not having any symptoms at all. If you have symptoms beyond the normal and expected, then please report them to v-safe or VAERS. There is a third path, called CISA that is initiated by a physician or health department.

“v-safe” is considered active surveillance - they text you every day with a link to update them on your symptoms, including reporting anything beyond the expected. VAERS is passive surveillance - anyone can report into it and it’s whatever comes in. It serves as an early warning system if something is wrong, but these are unsubstantiated reports. CISA is investigations that begin with a physician or health department and focus on an individual person with a complex situation that is not easily answered by existing guidance and information from the Advisory Committee on Immunization Practices.
What about NSAIDs?
NSAID stands for non-steroidal anti-inflammatory drug and includes things like ibuprofen (Motrin) and naproxen (Aleve). Some folks have heard about the reactogenicity associated with the COVID-19 vaccines and preemptively taken NSAIDs prior to their vaccine appointment. It’s best not to do this, if you can help it. BIG DISCLAIMER HERE: if you are under treatment by a physician for an unrelated medical condition and your dosing schedule happens to precede your appointment, follow your doctor’s recommendations. But if you are generally in a good state of health and wouldn’t normally be taking that pain medication, try to wait until you actually start having symptoms. The reason being is that as the name suggests, these drugs will dampen your inflammatory response - the things I wrote about earlier in this section. That makes you feel better, of course, but it might diminish your response to the vaccine too, in theory. Why go through this effort not to have the best immune response you can have, right? So don’t be afraid to take the NSAIDs if you feel you need them (i.e. if symptoms materialize) but it’s best to avoid taking the medication preemptively.
If you did do this prior to your appointment, you likely don’t need to repeat the series or anything. I don’t recall seeing data that specifically links NSAIDs use to diminished response specific to these vaccines. But based what we know about these drugs and how they work, it’s possible that they might counteract your immune response.
When might we expect vaccines for kids?
The Advisory Committee on Immunization Practices has asked the same question and here’s a slide from their 27Jan2021 meeting.

It appears that studies have already begun for adolescents (probably defined as 12 - 15 or 12 - 17 depending on the manufacturer) for Pfizer and Moderna. Johnson and Johnson (shown as Janssen in the table above) indicated that they were starting with adolescents 4-6 weeks after the adult results were ready and they just submitted for adult EUA a couple weeks ago. So they are probably enrolling adolescents now. For younger children, all of the manufacturers are probably enrolling them now since it says early 2021. We do have a possible head start with this population though for the Johnson and Johnson vaccine. This vaccine platform (an adenovirus vector) has previously been tested in children (infants - teens) and approved for use by the European Union. The only thing that is changing is the piece of DNA that the vaccine holds. The previous vaccine is for Ebola. The current vaccine in development is for COVID-19. Their previous safety successes with children for preventing Ebola might suggest that these vaccines will be successful in COVID-19 studies too.
Given the pace of the adult trials, we might expect to see at least one vaccine manufacturer submit data for EUA for adolescents and teens by the end of the summer. For younger children, I think it would be more like the end of the year or early 2022. But I should note that I have no inside knowledge on this or the success of these trials in progress. It is a guess based on what we’ve seen happen so far.
To me, this pandemic won’t really be over until my kids and kids around the world are vaccinated against COVID-19. But the light at the end of the tunnel is getting brighter and closer with each passing day.
Future topics
As you can imagine, I’ve received A LOT of questions. There was a lot to vaccine logistics so it took a longer time to get through that topic area. I’ve organized the questions into topic areas that I will address in upcoming newsletters:
Our path back to “normal.”
How long does immunity last?
Long term effects of the vaccines
Adverse reactions
Special populations and their risks and benefits of vaccination: autoimmune disorders, people with a history of allergies, pregnant/lactating women, and those who are trying to conceive
The list above does not indicate any rank of importance or the order in which I will answer them. I just want to let you know what’s coming in case you have a similar question. If you have a question that doesn’t align with the topics listed above, please email me.
Georgia
Testing
Guess what?! DPH finally updated their daily situation report to include antigen cases in their testing section (with a percent positive!!!) and in their maps and graphs. However, we still don’t have demographic data for antigen-positive cases. Hopefully that will come at some point.
Today there were 24512 newly reported PCR tests and 19304 newly reported antigen tests. For PCR tests, 7.6% were positive and 7.7% of antigen tests were positive.
Cases
There were 2174 newly reported PCR cases and 1505 newly reported antigen cases today for a combined total of 3679. The statewide 7-day case rate per 100,000 has dropped 71% since the winter surge peak, but remains 160% above the pre-winter surge base. It just goes to show how big the winter surge really was.
Hospitalizations
Today there were 261 new hospital admissions for COVID-19 and 29 admissions to the ICU. Statewide, 84 - 86% of the ICU beds are in use depending on whether you look at the DPH or HHS numbers, respectively. Hospital Region E (Athens-Clarke County and surrounding counties) is using less than 90% of their ICU beds for the first time since 26Nov2020.
Deaths
Today there were 172 newly reported confirmed COVID-19 deaths and 35 probable deaths for a combined total of 207. Thirty four percent of today’s confirmed deaths came from nonrural counties outside of the Atlanta metro, 28% came from Atlanta suburbs and 22% came from rural counties.
References
https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/downloads/prep-and-admin-summary.pdf
https://www.fda.gov/media/144414/download
https://www.fda.gov/media/144638/download
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-01/10-COVID-Oliver.pdf
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2020-12/slides-12-11/COVID-04-Oliver.pdf
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-01/04-COVID-Erbelding.pdf
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.