The Daily Digest, 18Dec2020
Georgia COVID-19 Updates

Vaccine Update
Today I’m planning to teach you about how the COVID-19 vaccines by Pfizer-BioNTech and Moderna. This is going to require us to dust the mental cobwebs of what we learned in high school (and perhaps college) biology classes. But I promise to keep things as simple as I can.
Cell and Molecular biology
Cell and molecular biology are huge fields and we are only going to scratch the surface of them today because, after all, this is not a biology course. You might know that your body is made up of cells and your cells contain a nucleus (purple ball inside the cell in the image below). That nucleus is where your DNA is stored, the genetic material you inherited from your parents. The DNA is the master instruction manual for every protein your body will ever need to make. It is found in every cell of your body, but only certain genes are activated (or turned on) for certain cells. For example, your liver cells don’t need to make the proteins that make up the unique structures of your eyeball. The process of taking the DNA instructions and making proteins with them is called gene expression.

Gene expression doesn’t go straight from DNA to protein though. There’s an intermediate biomolecule called mRNA (“m” = messenger). Structurally, it’s very similar to DNA. But unlike the double helix you’ve seen for DNA that provides a lot of stability, the mRNA molecule is single stranded, more like a string than a ladder. Because of this, mRNA molecules are really unstable and are easily degraded. mRNA is like the snapchat of a molecular message - a short-lived set of instructions. But the mRNA acts as a middle man of sorts between the master instruction manual (your DNA) and the ribosomes in the cytoplasm of your cells. Cytoplasm is just the liquid that is inside your cells that’s outside of the nucleus. Ribosomes are the protein builders. They “read” the temporary RNA message and then use that code to put the right building blocks in order to make the protein of interest. Keep in mind that the master instruction manual (DNA) and the builders (ribosomes) are held in different parts of the cell - we’ll come back to that. We just need temporary copies of the instructions so the ribosomes can do their job. The process of making this temporary copy of mRNA is called transcription. The process of taking the temporary mRNA message and making protein (the action of the ribosome) is called translation. It is called “translation” because you are converting genetic language into protein language.

This process of DNA -> RNA -> protein is referred to as “The Central Dogma” of molecular biology. Every living cell does this process and it always, always, always proceeds in this order. Notice that the arrows for transcription and translation are unidirectional. You can not go backwards in this process and make RNA from protein, for example. Remember I said all living things follow this sequence and never go backwards? There are certain viruses that can convert RNA to DNA, such as HIV. But there’s a debate whether viruses are technically living things, since they can’t replicate on their own - they have to hijack a cell in order to reproduce. So technically, it is still correct to say that no living thing violates the Central Dogma. In any case, neither does SARS-CoV-2, the virus that causes COVID-19. Nor do any of your cells.
Stability of RNA
Like I described in the section above, RNA has some structural features that make it really unstable. In fact, I spent five years isolating and working with RNA from bacterial cells during my graduate work. I can tell you from personal experience that it is an absolute pain to work with. It has to be constantly held on ice, in just the right solution, and it degrades very rapidly once it is removed from a cell. For example, whatever I hadn’t used in my experiments after a week was thrown out, because by that time it was worthless, even if held in cold temperatures. Compare that to working with DNA (remember this is double stranded and more stable). This molecule, once isolated from a cell, could be stored in a standard refrigerator freezer for months. But this helps us to see why the RNA vaccines from Pfizer-BioNTech and Moderna have a cold-chain requirement. They have to be held at cold temperature until they’re prepared for administration to vaccine recipients because the RNA itself is an unstable molecule.
The RNA vaccines
I recognize that not everyone is the sort of learner who understands from reading. The Journal of the American Medical Association has put together this helpful video to educate us on how the RNA vaccines (and all the COVID-19 vaccines in development) work. However, I will note that the video is a bit outdated and the concerns they had about whether the RNA vaccines would work have been overcome with the Phase III clinical trial data.
But for those who do better with reading, here goes. The RNA vaccines do not contain the virus genome or its spike protein. Instead they have a piece of RNA that codes for the SARS-CoV-2 spike protein that coats the outside of the viral particle. In the vaccine, those spikes aren’t present and the RNA is held inside of a pretend virus particle with a lipid membrane that looks kind of like our cell membranes (see “lipid coat” in the graphic below). So when the vaccine is administered, there is no virus in it at all, just the short-lived instructions (called mRNA) for how to make the spike protein. When the vaccine particles arrive at your cell and the cell brings them in, the RNA is released from the particle and runs into the ribosomes that are in the cytoplasm. Ribosomes don’t really discriminate mRNA messages - as long as they have the right chemical composition at the beginning of the sequence, the ribosomes use them to make proteins, whatever the mRNA (temporary message) says. So the ribosomes aren’t paying attention to what is my mRNA versus the vaccine’s mRNA. The spike protein is then produced by the ribosomes in the cytoplasm of the cell and then presented on the membrane of the cell by the “name tag” holders of the immune system. From our last lesson, every cell in your body has a name tag holder (technical term is MHC molecule) that shows either your proteins (called self-antigens) or something they found in their cytoplasm (foreign antigens). If the immune system cells that surveil your body find a name tag (foreign antigen) that they don’t recognize, then they send out the alert and this recruits other immune system cells so they can learn about the new threat and develop antibodies and memory against the threat. So the bottom line is that the vaccine is taking a temporary, short-lived instruction set for making the virus spike protein and getting your cells to make the protein temporarily. And this spike protein is a foreign antigen, it has the wrong name tag in my analogy. Your cells show the spike protein to your antibody producing cells (there are several intermediate steps here, I’m simplifying) and they recognize that it is not a self antigen. So they begin to produce antibodies. Both the mRNA that was in the vaccine and the spike protein we produce from it will degrade over time, but the memory remains. So I called this vaccine’s mRNA like a snapchat, but it’s also kind of like the messages sent in the movie/show “Mission Impossible”: this message will self-destruct in 5…4…3…2…1. Meanwhile, your cells now know their mission.

So let’s address some of the safety myths with this mechanism of action in mind. Can the vaccine give you COVID-19? Absolutely not. The vaccine does not contain the virus, nor its genome or proteins. The only thing it has in it from the virus is a temporary copy of the instructions to make just one of the viral proteins. Can the vaccine alter my DNA? Highly unlikely - your DNA is held in your cell’s nucleus (the purple ball in the first diagram). The vaccine mRNA has no reason to enter the nucleus - it has no purpose there because the ribosomes that translate mRNA into protein are in the cytoplasm. In essence, your DNA genome (your master instruction manual) is sequestered away from the action. Generally speaking, mRNA is made in the nucleus (transcription) and then leaves the nucleus immediately to be processed by a ribosome. RNA does not re-enter the nucleus. This compartmentalization of the processes makes it very unlikely that the mRNA in the vaccine ever enters the nucleus and therefore it never is in close proximity to the genome. In addition, the cell has no mechanism by which to convert the vaccine mRNA into DNA to then insert into your genome - remember your cells follow the Central Dogma.
Testing
It was a big day for testing for Georgia, with 47,876 new PCR test results reported through Electronic Laboratory Reporting (ELR). Of today’s tests, 13.3% were positive. The Georgia DPH does not provide similar data for antigen testing. However, the antigen test identified 25% of today’s net increase in total cases. Last week, we broke the record for most PCR tests performed in a single week for Georgia. This week so far, we’ve already met the total test output of the week before that record-breaking week. I’m not sure we’re on pace to set a record this week.
Cases
It was a record-setting day for newly reported cases in Georgia. Compared to yesterday’s totals, there was a net increase of 6092 PCR-confirmed cases and 2049 antigen test-identified cases for a combined total of 8141 for the day. The state’s 7-day case rate per 100,000 residents using PCR + antigen cases is now 69% higher than the peak we experienced in the summer.
As I’ve discussed previously, the Georgia DPH does not include antigen cases in any of their graphs or maps, despite the fact that they investigate every antigen case the same way they investigate PCR cases and the fact that in high disease incidence areas (i.e. Georgia and the US) the antigen test is as good as the PCR test at identifying positive cases. The exclusion of the antigen case data from the data visualizations on the DPH website can give people a false sense that the situation is not that bad. Below, I’ve provided a side by side look at the maps using the DPH method (PCR cases only) and adding the antigen cases (right side). The color coding break points are as similar as I can get them. I recognize that the images will appear very small in the newsletter. You can review the maps more closely and click/hover on your county of interest by consulting the DPH daily status report and this link to my purple map.

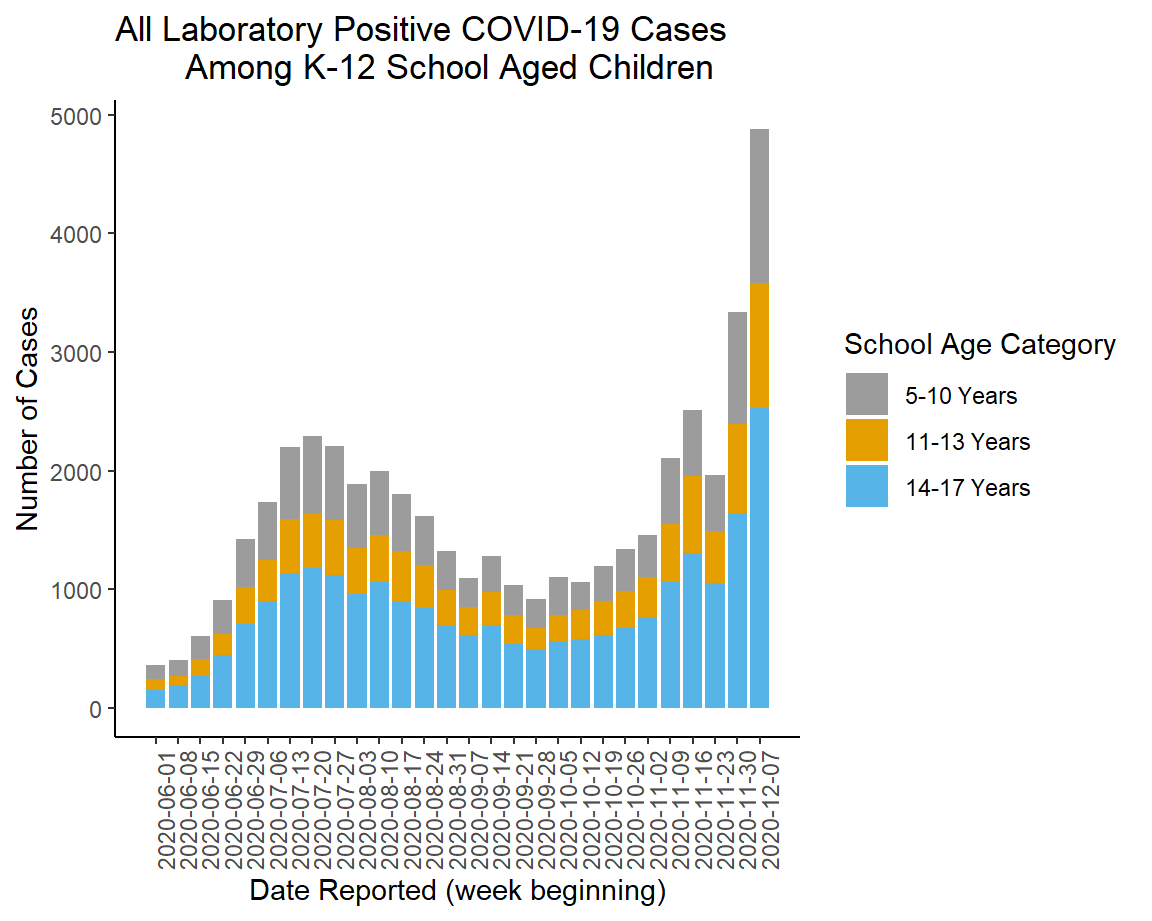
The other thing of note today is the release of the School Aged Surveillance Data report. Below we can see how cases among school-aged children have varied over time, using both PCR and antigen cases. You can see that we have seen a dramatic escalation of cases among K-12 aged children and the summer surge is but a minor bump now. To be clear - these aren’t necessarily cases linked to a K-12 setting, but rather cases among children (statewide) who are in these age groups.
If we look at the wider population, using both PCR and antigen cases adjusted for population of each age group, the graph below shows us how things are trending now. Children are represented in this graph by the yellow line. College aged adults and all adults 23+ have a near identical case rate increase over the past two weeks.

Looking at the 7-day case rate for each county type over time, we can see that so far, there are increases for every county type but they are comparatively smaller for the Atlanta counties of Fulton and DeKalb. The other three county types (Atlanta suburb, rural and nonrural) are all grouped together. Ignore the spike around early October - that’s a data dump of ~26,000 antigen cases that DPH shared, all at once.

Taken together, the data show that the case rate increases are affecting every county type in the state, every region of the state, and every age group of the state. We all need to do more to limit transmission in our communities.
Hospitalizations
The Georgia Geospatial Information Office hospital dashboards are back online. But I will say that the data look wonky for ventilator usage over time, where it shows a substantial increase over the past couple days. From the announcement on the GIO data hub, it seems there may have been some errors with the ventilator data. But it’s unclear if the error is the recent data or the historical data.
Today, there were 346 new hospital admissions for COVID-19 illness. We’ve had four 300+ admission days in a row now, so it’s clear that this is going to be a big week for hospitalizations. There were also 42 new COVID-19 admissions to the ICU. According to the GIO dashboards, 35% of adult ventilators are in use. This number had consistently been 31-32% over the past two weeks. But as I said above, I’m not really sure what to make of this increase yet. Only 14% of the state’s ICU beds are unoccupied as of today. The large numbers of hospital admissions this week might mean greater demand for the ICU next week as the condition of some of these newly hospitalized patients deteriorate.

As of today, there are 6 of Georgia’s 14 hospital regions that have more patients in hospital now than they did during their highest point in the summer surge. They are regions A, B, C, E, G, and N. These are all in the northern part of the state.
Another piece of interesting information from the School-Aged Surveillance Data report is the continuing growth in ER visits among children and college-aged adults for COVID-19 illness. So we aren’t just seeing increased cases among children, we are seeing increases in the number of cases that require emergency medical attention.

Deaths
There was a medium-low number of confirmed deaths reported today, 38. The updated statewide total is 9396 for confirmed deaths. The 7-day death rate per 100,000 across all county types for Georgia is shown below. So far, we have mercifully not seen the surge in deaths following the surge in cases. We see some increase since the beginning of December, but it’s too soon to see if this is just the noise of day to day and week to week variation or the beginning of something bigger. Hopefully not.

It’s been a great week in many ways with the vaccine roll out. You can see DPH commissioner, Dr. Kathleen Toomey, receiving her vaccine here. Her excitement and relief is also how I feel and what I’m hearing from many colleagues in the medical field. In fact, my sister who is a doctor here in Kansas received her vaccine today. Our family text thread of parents and siblings was a very exciting place as we celebrated.
But it’s also been a tough week for Georgia, with record setting days for cases and surges in hospital demand that was made worse by the fact that we were flying blind for part of the week when the hospital dashboards went down. The data show that the case surge is across the state and for every age group. It is incumbent on all of us to do our part to limit transmission to the greatest extent possible.
References
https://www.cas.org/blog/covid-mrna-vaccine
https://edhub.ama-assn.org/jn-learning/video-player/18547208#
https://dph.georgia.gov/covid-19-daily-status-report
https://datawrapper.dwcdn.net/3isaj/1/
https://covid-gagio.hub.arcgis.com/
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.
Thank you so much for your podcast and updates. I'm a fellow virologist and it has been tremendously comforting to have your site for reference when I do not have the energy/effort to explain. Beautiful graphics and updates.