
I just got in from shoveling snow off the driveway, outside of Kansas City. So all of these images from Tampa for the Superbowl are making me jealous. I want to remind folks to be cautious about gathering for the game today - it’s best to just watch with your immediate household or bubble. Go Chiefs!
Combined Data
The graph below shows how four of our big metrics for tracking the COVID-19 pandemic are tracking over time. Cases are represented by the blue line and correspond with the left y-axis. All other metrics correspond with the right y-axis. The reason I graph all of these things together is so that we can see the way these things trend together (or differently) over time.

This week we are continuing to see cases decline for COVID-19, by 11%. Hospital admissions also decreased, by 13.3%. ICU admissions held steady this week. Deaths have also held steady.
Testing
This week we a 13% decrease for PCR tests performed. In total, there were 211,530 PCR tests reported. Of those, 11.7% were positive. The test output trend over time can be seen in the graph below, represented by the blue line that corresponds with the left y-axis. The red line represents the test positivity rate over time, and corresponds with the right y-axis. The gray dashed line is the goal line for test positivity.

The percent positive rate has decreased, but we still remain far above the 5% goal line. All the same, it’s good to see the number trending downward.
The Georgia Department of Public Health does not provide data regarding the number of antigen tests that have been performed nor how many were positive. Further, they do not provide any demographic details for cases identified by the antigen test. Keep that in mind as we go through the demographic data in the following sections. You’re only seeing part of the data. Meanwhile, antigen testing identified 27% of the cases this week.
Cases
The number of combined new cases (by date of report) is as follows:
- 24 hours: 3153 by PCR + 436 by antigen = 3589 (+0.4%)
- 7 days: 23,111 by PCR + 8,435 by antigen = 31,546 (+3.5%)
- 4 weeks: 136,605 by PCR + 47,341 by antigen = 183,946 (+24.3%)
The new statewide total is 940,991, combining PCR and antigen-test identified cases. Bear in mind that as large as these case totals are, they are likely an under count of our actual case count - it’s a problem that plagues public health for multiple diseases and especially so when a disease has so many asymptomatic cases, as COVID-19 does. But also because we know that our percent positive rate is high. So there are likely a fair amount of cases out there that we are not detecting. In the graph below, I show the Georgia cases by date of report for both PCR and antigen cases for each county type. Ignore the big bump around 11Oct - that was a data dump of antigen cases. You can check how your county is classified here.

The next two graphs show us some of the demographic details of those who are getting sick and testing positive. In each graph, you’re looking at 8-week timelines for each age group side by side.

This week we saw decreases in cases for every age group except those <1. However, cases are still quite high. Cases are also decreasing for every race as well as the “unknown” category. That’s an indication that contact tracers are better able to manage the workload as cases have decreased.
Hospitalizations
The number of combined new hospital admissions (by date of report) is as follows:
- 24 hours: 110 new COVID-19 admissions, 8 admissions to the ICU (weekend reporting is typically light)
- 7 days: 1605 new COVID-19 admissions, 199 ICU admissions
- 4 weeks: 7207 new COVID-19 admissions, 856 ICU admissions
The state’s dashboards for patient census and hospital capacity are back up and running for now. They indicate a big drop in the number of patients currently hospitalized - 3456. I’m hoping to check that against the US Department of Health and Human Services data when it is updated tomorrow. Because the HHS data shows a much higher number than the state. One possible explanation for that difference is the inclusion or exclusion of pediatric hospitalizations. The HHS data include pediatric data. If those numbers are subtracted from the HHS total, then the number more closely resembles the state number. So I’m not sure if Georgia isn’t including pediatric hospitalizations in their reporting. I’m working to get clarification on this.
As mentioned in the combined data section, hospital admissions for COVID-19 decreased this week, but ICU admissions were nearly the same as the previous week.
The graphic below shows us the Georgia Emergency Management Agency hospital regions. The table on the right tells you how each region is doing with respect to usage of their available ICU beds and how their COVID-19 patient population compares to their overall patient population.

There’s a LOT of news to celebrate here, even as we still see a lot of red. First of all, take notice that there are only 2 hospital regions using >90% of their ICU beds (regions E and N). The graph below shows you how this compares to our history since Labor Day. We’ve certainly been through a huge challenge. But things are returning to the pre-surge baseline. In addition, if we look at the patient census we now have 5 regions in the light red zone and one zone (L) in the orange zone. As recently as 18Jan, all regions were in the dark red zone. Region L is the closest region to reaching its pre-surge baseline. Many others are not far behind.

As a reminder, hospitalizations are down - yes. But they remain very high. We need to continue to do the long, difficult work of limiting disease transmission to give our healthcare workers the space they need to do their jobs well and to give them time to recover.
Next, let’s look at the demographic details that we have for hospitalizations.
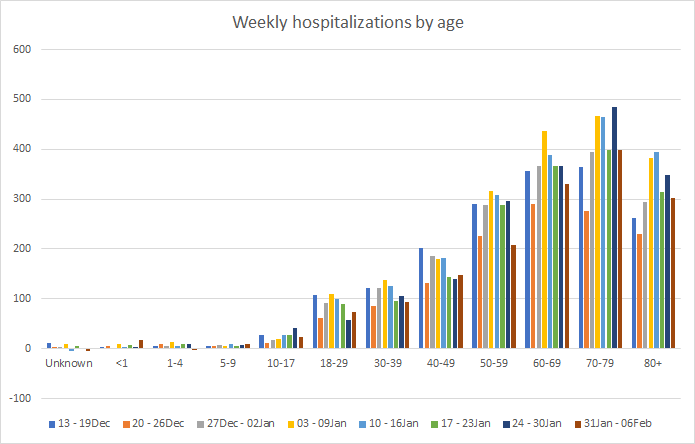
This week we saw decreases for many age groups. The exceptions are children <1 and 5-9, 18-29 and 40-49.
If we look at ICU admissions by race, things have come down a long way for White populations. However, in the most recent week we’ve seen increases for those who are Black / African-American and “Other.” The “other” category includes the majority of those who identify as Hispanic/Latinx. So we’re seeing a growing need for ICU beds among people of color.

In Georgia, the COVID-19 hospitalization rate, on average, is 5.5%. For those who are hospitalized, 16.6% require an ICU bed. While the case fatality rate for confirmed cases and confirmed deaths right now is 1.73%, the fatality rate for people admitted to the ICU for COVID-19 is 39.9%.
Deaths
The number of new confirmed deaths (by date of report) is as follows. The percentage in parentheses indicates how the increase compares to Georgia’s cumulative total at the start of each window of time.
- 24 hours: 2 (+0.02%)
- 7 days: 756 (+6%)
- 4 weeks: 3044 (+29.6%)
This week the number of deaths was nearly the same as the previous week, with only a 1.7% reduction compared to the previous week. The current statewide total of confirmed deaths is 13,326 and of those, 22.8% were reported in the last 4 weeks alone. That means that more than one out of every five deaths Georgia has recorded since the start of the pandemic was in the past 4 weeks - it’s a lot of death. The graph below shows how the 7-day death rate per 100,000 residents has trended over time for each county type. The state death rate is 51% above the peak during the summer surge. The death rate is worst for rural counties and best for the Atlanta counties of Fulton and DeKalb. In fact, the death rate in rural counties is 67% higher than the death rate in Atlanta.

Next, let’s look at the demographic data for this week’s deaths. Deaths increased for those 18-49 and 60-79. Deaths decreased for those 50-59 and 80+.

Yesterday we unfortunately set a new record for confirmed deaths reported in a single day, at 178. Let’s take a deeper look at the disparities that are happening between county types based on cumulative data. First, let’s begin with a comparison of the average (mean) age of death and median age of death. The median is less susceptible to outlier numbers and represents the middle-most number in a series of numbers.

The median age of death is the same for all county types other than nonrural counties, which are older. However, if we look at mean age of death, the deaths in Atlanta suburb counties are the youngest. Atlanta and rural deaths have about the same mean age of death. If we adjust for population, here’s how the county types compare for each age group. You can see that rural counties are dominant starting with the 30-39 year group onward.

If we consider race, non-Atlanta metro deaths are typically Whiter than Atlanta metro counties. People of color make up a greater proportion of deaths in Atlanta and Atlanta suburb counties, but especially Atlanta counties (Fulton and DeKalb).

If we look a little closer at Atlanta deaths, we can see that the deaths among non-White populations are dominant throughout all age groups except for 0-19 and 90+. Note that these are total counts, not adjusted for population.

Compare that to what’s happening for rural deaths. Here, deaths among non-White populations are dominant for ages 20 - 49, but the majority of deaths are among White populations for all other age categories.

It is not really news that the pandemic is being experienced differently in Atlanta versus rural counties. So far, when adjusted for population, Atlanta is experiencing a lower death rate than rural counties. However, the people who are dying in these two county types are very different.
That’s it for this week. I’ll be back tomorrow to put the Georgia pandemic in the national and global context. Go Chiefs!
References
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.