The Sunday Week in Review, 10-16Aug2020
Georgia COVID-19 Updates

The 14 day window of uncertainty
Recently, Governor Brian Kemp has made some statements that have brought the 14 day window of uncertainty back into the forefront. For people who have followed this newsletter for a while and feel confident about what the 14 day window is (and isn’t) then feel free to scroll through this next section. But I want to make sure everyone understands the significance of this window of time. Here’s what the Governor had to say in his press release. The screenshot is from WSB-TV.

The area boxed in yellow is problematic with errors in every sentence. Cases have dropped in the past 14 days, but only if you are looking at the cases by date of symptom onset. And the past 14 days are the window of uncertainty. More on that below. The Harvard Global Health Institute ranks Georgia today as the highest state in the nation for average daily case rate per 100,000 residents. So characterizing our rate of transmission as “low” would be laughable if we didn’t have so many people dying preventable deaths right now. In fact, the Harvard tool indicates that 156 of Georgia’s 159 have such widespread community transmission of COVID-19 that it warrants a shelter in place order to bring transmission back to within manageable levels for testing and contact tracing. The mortality rate did fall once the case surge began in late June. But that descent has plateaued over the past two weeks. If our deaths continue to climb, we might expect to see that case fatality rate begin to increase again.

Let’s move on to the 14-day window of uncertainty. Below, I’ve included a slide showing the two different ways of graphing cases on the Department of Public Health COVID-19 daily report with pros and cons of each method. The graph the governor is referring to is the one on the left, graphing by date of symptom onset. Note that there is a vertical line at the 14 day window, after which the data are subdued and not connected to the rest of the graph.

Why do we have a 14 day window of uncertainty? Because in infectious disease, it is unusual to know who is sick in real time. I’ve built a timeline of a person’s disease course and how it relates to the graph by date of symptom onset below. The ranges and timing are based on guidance from the CDC and a recent report estimating the testing turnaround time, on average. First, a person will not go seek medical care the first day they have symptoms. One might think it’s allergies, or a common cold, or try to ride it out at home. But eventually, they might seek a doctor’s appointment and/or test for COVID-19. Then, once the specimen is collected it is estimated to take 4-14 days based on a recent report for that test result to be reported. Once the case is reported to the state, it is backdated based on the date on which a person first started experiencing symptoms. Using the mean days it takes from symptoms to test collection, a case can be backdated 10 - 20 days from the date on which the result was reported. This is why the 14 day window exists. You can see how backdating is taking place for Georgia here.

The cases will always appear to be in decline in the most recent 14 days because of the timeline above. After all, the chances of a person developing symptoms today, seeking a test today, and getting their test result today are very, very low - even before our testing backlog began. So for the Governor to reference this decline as a positive sign shows that he either doesn’t understand his own data or he is betting that the average Georgian doesn’t understand how this graph works. Either way, we need to be making data-driven decisions when it comes to a scientific problem like the pandemic.
Let’s move on to this week’s review.
Testing
Test capacity is strained across the nation because of increased demand for tests, as community transmission continues to intensify. There are shortages of the supplies and laboratories might be hitting the maximum throughput they can achieve but it isn’t meeting demand. In fact, this week the White House Coronavirus Task Force report on the states suggested that Georgia should effectively commandeer university laboratories to conduct testing to support K-12 and community college testing as well as to monitor university populations.
It appears that the state has made efforts to try to expand testing by contracting with out-of-state labs, but disconnects in communication infrastructure are holding the state back from success. As a reminder, infrastructure cannot be built overnight, even in a pandemic. So the fact that the Department of Public Health relies on antiquated reporting mechanisms is a consequences of years of poor funding for public health. Even this year, in the midst of the pandemic, the Department of Public Health took a budget cut along with the rest of the state agencies. The state is depending on the federal government for the test kits that are used by public health districts as well as shipping costs. If federal money runs out for Georgia’s pandemic response, the testing woes we are experiencing now will only get worse. And that is the very last thing we want heading into influenza season.
A week ago, we set a new record for total tests performed in a week’s time. But our testing output this week is far below that previous record. It’s actually at a level we haven’t seen since mid July, as the case surge was intensifying. Of the 17,207 new tests reported today, 10.6% were positive. The weekly total is 170,225 tests and a weekly percent positive rate statewide of 9.4%.

Cases
In the first graph below you'll see cumulative cases to date broken down by county type. Previously, I’ve shown this graph since the beginning of the pandemic, but I have since truncated it to when we reopened the state on 24Apr. I've marked the last four weeks with blue arrows.
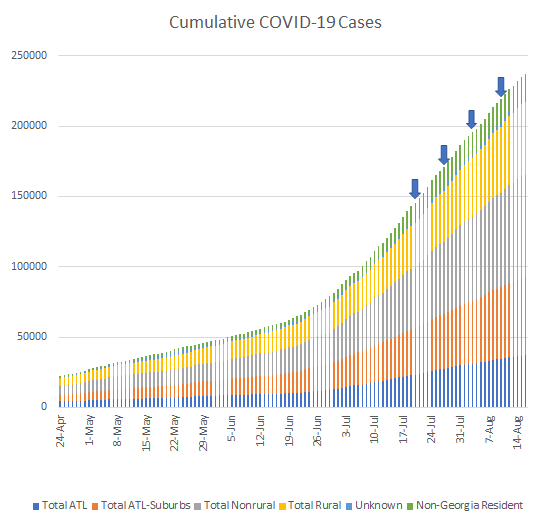
The number of new cases (by date of report) is as follows:
- 24 hours: 1862 (+0.8%)
- 7 days: 20,434 (+9.4%)
- 4 weeks: 93,907 (+65.6%)
The new statewide total is 237,030 which means that of all the cases that have been recorded, 39.6% were reported in the past 4 weeks. That is a lot of growth, but this rate over the past month has been decreasing, week by week, as cases have appeared to level off. I certainly hope that the case leveling is real, but I suspect that testing backlogs are hindering our ability to track and monitor cases to the best of our ability. I discussed the testing backlogs above and in the past and I don’t think this leveling is real, but rather an artifact of our intense testing backlogs.
From the case bar graph you can see that I often break cases and deaths down by county category. But considering there will be very disparate population densities in those areas, it’s important to see how intense disease is in these counties when adjusted for population. By county type, the cumulative case rate per 100,000 is as follows:
Atlanta: 2177
Atlanta suburbs: 2074
Nonrural: 2182
Rural: 2348
From the beginning of the pandemic to now, rural counties are being hit harder than any other county type. That’s despite having a lower population density and thus less opportunity for the disease to spread. Compared to the next highest category (nonrural counties), rural counties have a case rate that is 7.6% higher.
Below is a breakdown of how new cases were distributed by age this week (red) compared to last week (blue). There are decreases in most categories. But there are increases in those 5-17 years old (school aged children) and those 70+.

Hospitalizations
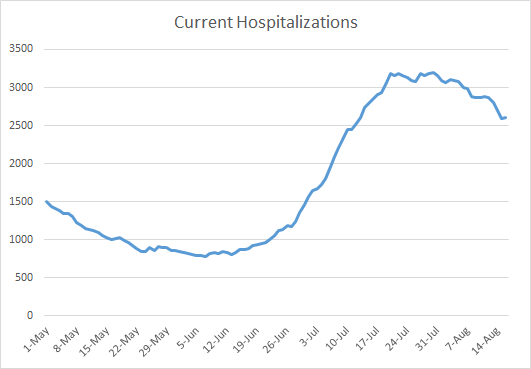
Here is where current hospitalizations are. They have declined over the past two weeks, a sign of hope. Let’s hope that trend continues.
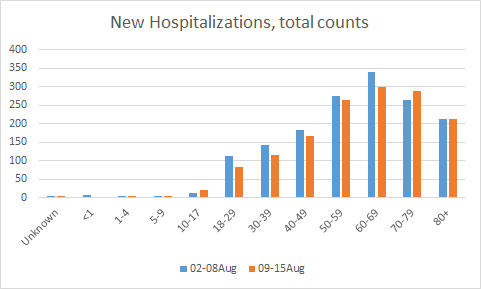
Here is how new hospitalizations this week compare to last week, broken down by age. There are decreases in many age groups but there are increases among those 10-17 years old and 70-79.
Deaths
The number of new deaths (by date of report) is as follows:
- 24 hours: 33 (+0.71%)
- 7 days: 503 (+12.0%) <- a new record
- 4 weeks: 1,529 (+48.2%) <- a new record
The new statewide total is 4,702 which means that of all the cases that have been recorded, 32.5% were reported in the past 4 weeks. So our deaths are accelerating as we saw our cases accelerate last month. Deaths are a lagging indicator compared to cases. So we will have a better sense of whether our current “decline” in cases is real depending on what happens with deaths. If the deaths continue to climb, it likely means that cases have also been continuing to climb (to feed that climbing death rate) but we weren’t able to properly see them due to problems with testing output. Our deaths have increased by nearly 50% in the past month alone. As for cases, I’ve calculated the cumulative death rate per 100,000 based on county type.
Atlanta: 43.4
Atlanta suburbs: 37.1
Nonrural: 44.1
Rural: 62.8
Rural counties are dying at a rate that is 44% higher than the next highest county type (nonrural counties).
There’s also something interesting going on with the deaths reported to date for the past couple months. The mean age of death is steadily declining and that’s interesting since in the early stages of the pandemic so many of our deaths were among the elderly. In other words, our deaths are trending younger.

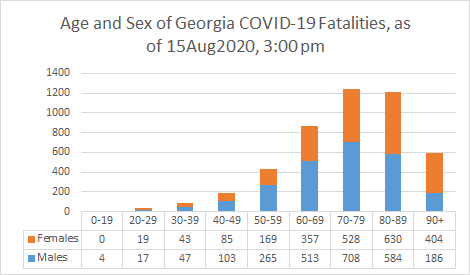
Here’s how Georgia fatalities have broken down by age and sex.
And here is how fatalities have been distributed by age and race.

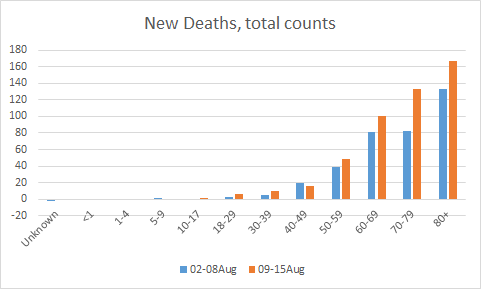
Finally, here is how deaths this week compare to the previous week, broken down by age. There are concerning increases for everyone above the age of 50.
Combined Data
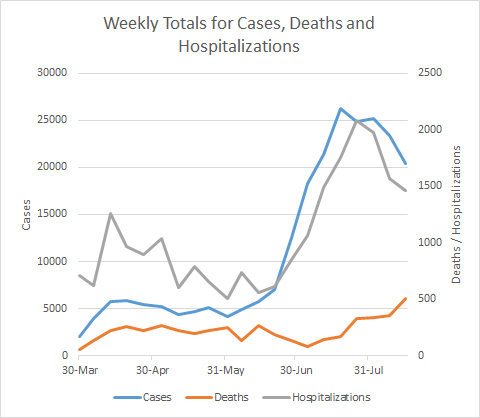
Below is a graph that allows us to see weekly trends for cases (left y-axis) and hospitalizations and deaths (right y-axis). Cases and hospitalizations appear to be declining. Deaths are on the increase.
I’ll be back tomorrow with a look at how Georgia compares to the national context in this pandemic.
I’m still gathering kids questions on COVID-19 for this week’s episode of Public Health for the People. If you’re interested in submitting a question, please email amberschmidtke.phd@gmail.com.
References
https://dph.georgia.gov/covid-19-daily-status-report
https://globalepidemics.org/key-metrics-for-covid-suppression/
https://www.ajc.com/news/white-house-warns-of-widespread-and-expanding-viral-spread-in-georgia/5DEVU3BSCZAIHCSI3A3KTTGGIY/?fbclid=IwAR2COsoE9FYHQxnP8xZQ-7IImVU42u__DhPNvJ3_syuUTaIIyPjgwX-8vG0
https://www.11alive.com/article/news/health/coronavirus/coronavirus-numbers/backlogs-wait-times-and-technology-challenge-georgia-testing-goals/85-4c614f53-63cf-4049-b94e-94aa7b82485e
http://208.97.140.204:8080/epicurveInteractive-cases.html
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
Hi! I saw the FDA approved emergency use of saliva tests. Any idea when those tests could be available to the GA public? Are those fairly accurate? Thanks for all you do.