The Daily Digest, 27Jan2021
Georgia COVID-19 Updates

Public Health Advocacy
I have good news to share today. The Georgia House Appropriations Committee passed HB 80 this morning. From here it goes to a vote by all members of the Georgia House, scheduled for tomorrow. For public health, you can review the tracking sheet of what new money was proposed on pages 55-56. This bill includes state funding for the following:
Three new positions at DPH: a chief medical officer, a deputy commissioner and a chief data officer. A total of $286,000 has been proposed for these three positions.
$18 million to replace the GRITS system that is primarily used to track pediatric vaccinations but has been unable to meet the demand of tracking vaccinations in the COVID-19 pandemic. GRITS dates back to 1996 and is in desperate need of modernization.
$15 million to the AIDS Drug Assistance Program (ADAP). This program provides funds to provide medications to HIV/AIDS patients who might not be able to afford them. In case you didn’t know, Georgia is the state with the highest incidence (new cases) of HIV in the nation and this has been going on for years.
So if you have been contacting the House Appropriations subcommittee - great job! I mean, it’s possible that these representatives were already planning to better fund public health, but I’m sure your emails and phone calls made an impact too. Now is the time to send them a thank you message, but we also need to pivot to contacting the representatives from your district. Because they are voting on this bill tomorrow. You can look up that person here.
I should mention that this House bill is for the amended FY21 budget that runs through June of this year. We still have not heard about state appropriation changes from the Governor’s proposed budget for FY22 that currently includes only negligible funding improvements for DPH.
This issue has gotten a LOT of media attention this week, even as there are so many other important news items that deserve print and air time. This week, we’ve seen stories from the Atlanta Journal-Constitution, Atlanta Magazine, the Savannah Morning News. I’ve also been interviewed on this issue by TV news stations and other local newspapers whose stories are yet to be published.
Yesterday I wrote a Twitter thread on why public health needs to be funded not just during the pandemic (a band-aid) through temporary federal aid. But we also need sustained, long term investment using state dollars to improve public health and correct many areas where Georgia lags behind other states.


Vaccine Update
I’ll be quick in this section today, although there is a LOT to discuss here too since the Advisory Committee on Immunization Practices is meeting today to discuss updates on the currently available vaccines. You can review their slides or watch their presentations and discussion for now, but I will unpack much of this on Friday.
I do want to point out some news from Merck, a vaccine manufacturer (with a long, successful history in vaccine development) that was developing two candidate COVID-19 vaccines. Two days ago, they decided to discontinue their studies because the vaccine candidates did not show adequate efficacy (i.e. preventing disease) compared to natural infection or the already EUA-licensed vaccines (Pfizer and Moderna). This matters for two reasons: (1) it’s a reminder that we are VERY lucky to have two vaccines with ~95% efficacy; (2) it might provide reassurance to many that the vetting process for the COVID-19 vaccines is thoughtful and robust. Vaccines that don’t work or that have intolerable side effects do not advance through clinical trials and the FDA approval process. The fact that the Pfizer and Moderna vaccines did make it through these trials and approval process is a big deal.
It does appear that the White House Coronavirus Task Force reports will continue and today the Biden administration released the reports for all 50 states and US territories. This is a really big deal. I can’t tell you how many open records requests I’ve had to file for multiple states in the past year for these reports. Many states were responsive to my requests but a good chunk of them were not. In July, I requested the 50 States reports from the Department of Health and Human Services (Secretary Alex Azar was the chair of the WHCTF) and the FOIA request remains unanswered, six months later. And yet, these reports included important safety recommendations for the population. Not every state has had the funding for robust data dashboards. These reports were an important equalizer and it was deeply troubling and unfortunate that the American people didn’t have equitable access to COVID-19 data and safety recommendations. According to the 24Jan2021 WHCTF report, they marked that 1,235,775 vaccine doses had been distributed to Georgia, or 2.9% of all doses distributed in the US. Of that distribution, Georgia had used 534,161 doses to initiate the 2-dose series and 59,965 Georgians have completed the 2-dose series. In total, 48.1% of the state’s distributed doses had been administered. Of course, these numbers are already out of date, three days later. In addition, it’s not clear that doses distributed equals doses received by the state. But given the cold chain storage requirement, I don’t think these are the sort of things that get stuck in the mail. The US has given the first dose to 7.2% of the adult population and Georgia is not far behind at 5%. Georgia doubled its percentage in the most recent week.
Testing
Today was a lower output day for PCR testing, with a total of 24,499 new results reported through Electronic Laboratory Reporting (ELR). Of those tests, 15.6% were positive. A higher than usual amount of cases were identified by antigen testing today (36.2%). We do not get data on total antigen tests performed nor how many are positive.
Georgia’s test positivity rate (weekly) remains above the national average. However, the positivity rate is decreasing for both at a similar pace. Let us hope that trend continues.

Using the data provided in the 26Jan2021 HHS Community Profile Report (different dates than the WHCTF report), Georgia has the 6th highest positivity rate in the country. Part of that is explained by the fact that we are ranked #38 in the nation for tests performed per 100,000. This week, we moved up a spot when it comes to turning laboratory results around in 3 days or less. We are now ranked 46th in the nation (73% of tests). Having a rapid test turnaround time is important for getting compliance with isolation and quarantine instructions given to confirmed cases and close contacts. All but four states are above 90% for this metric, although California and Florida do not report data for this metric. So Georgia is not just low, but really low, for turning tests around quickly.
Cases
Today there was a net increase of 6384 newly reported cases (4074 by PCR and 2310 by antigen test). Of today’s newly reported cases, 37% came from nonrural counties outside of the Atlanta metro. Twenty seven percent came from the Atlanta suburbs and 22% came from rural counties. The graph below shows how our descent from the most recent peak is going for each county type.

We can see that the Atlanta counties are doing the best right now and the Atlanta suburbs have the highest case rate. The Atlanta suburb rate is also not decreasing as rapidly as the other county types.
As of the 24Jan2021 WHCTF report, Georgia is ranked #6 in the nation for new case rate per 100,000. There are 156 Georgia counties (of 159) in the red, orange or yellow zone.
Hospitalizations
Today there were 332 new COVID-19 hospital admissions and 42 admissions to the ICU. These are typical numbers for Georgia, based on recent trends. There are 4741 COVID-19 patients currently hospitalized. This is a further decrease compared to the most recent peak, but the descent is slowing down.
In addition, something weird is going on for hospital region J (Savannah and coastal Georgia) in the graph below. You’ll see that they’ve seen a significant bounce over the past three days. It’s too soon to know if this will be a sustained increase or a surge on top of a surge.

Here’s how Georgia hospital regions are doing with respect to ICU bed usage and the COVID-19 burden on their overall patient census.
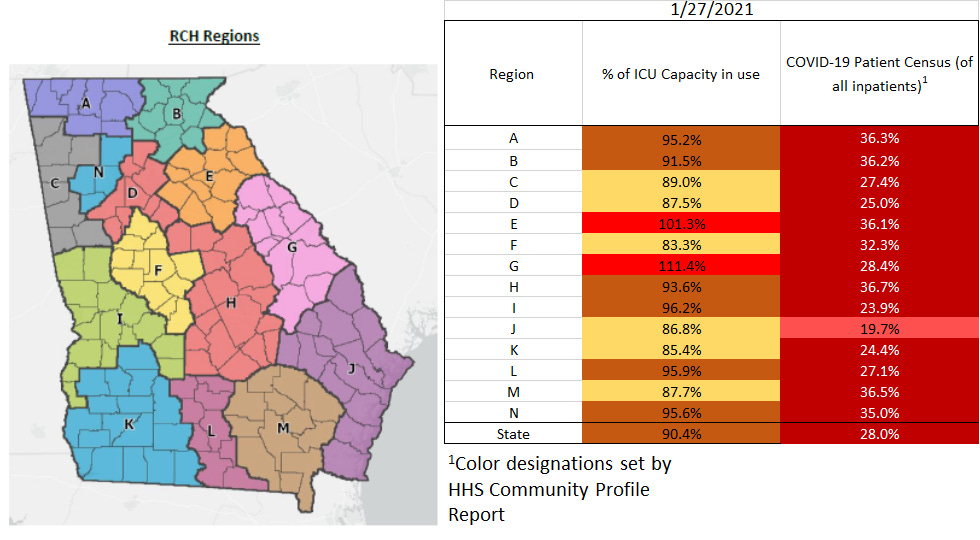
There’s good news again here with one fewer region using an overage of their ICU beds (region A dropped off today). However, region E and especially G continue to experience a lot of strain for ICU beds.
Using the data from the 26Jan2021 HHS Community Profile Report, Georgia is tied with Arizona for the #1 state in the nation for confirmed COVID-19 admissions per 100 beds in the past 7 days. We are ranked #3 in the nation for percentage of ICU beds that are occupied by COVID-19 patients (46%).
Deaths
Today there was a net increase of 139 confirmed COVID-19 deaths. Of these, 33% came from nonrural counties outside of the Atlanta metro, 29% came from rural counties and 24% came from Atlanta suburb counties.
Unfortunately, there is a new report of a pediatric death compared to yesterday’s report and I was able to confirm this with two contacts at the Department of Public Health. He was a 17-year old boy from Baldwin county. He is noted as having an underlying condition but we do not have details with respect to whether that comorbidity contributed to his death from COVID-19. His is the 9th pediatric death since the start of the pandemic. And if you’ll notice from the table below, six of those nine pediatric deaths have been among Black / African - American children. It’s just another reminder of the toll this pandemic is having on people of color.

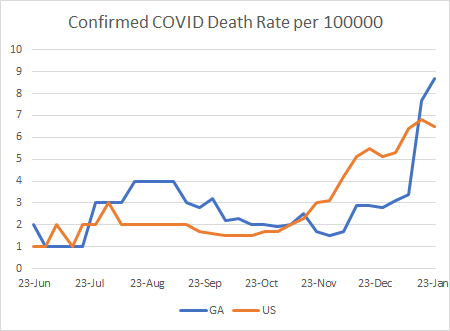
Using the White House Coronavirus Task Force report, we can see how the Georgia weekly death rate for COVID-19 has compared to the US trend over time. As the death rate seems to have peaked for the US, Georgia continues to climb. However, that climb is slowing down, so perhaps we are nearing the peak.
I talk a lot about the disproportionate amount of death that is happening due to COVID-19 in rural counties. But this map below really shows it in a way that the graphs can’t. These are new deaths per 100,000 in the past week. Yes, there are populated areas with higher death rates. But the majority of those dark red counties are rural counties.

Schools
I’ve been asked multiple times to weigh in on arguments for and against in person instruction in the K-12 setting. I have been reluctant to engage in local disputes but you are all welcome to use the data that I provide to make your arguments. Another reason for my reluctance is conflicting information. Case rates appear to be lower among children than other age groups. But we also know that children have the highest test positivity rate (see green line in the graph below), meaning that we aren’t testing them widely enough and it’s not even close to the positivity rate for other age groups, especially in the fall/winter surge.

But yesterday the CDC publicized a study with the graphic below that demonstrated that having a strong safety culture in the K-12 setting resulted in very limited disease transmission in schools. They also wrote a “viewpoint” article in the Journal of the American Medical Association, akin to an op-ed in academic and medical journals.

I’m going to highlight two paragraphs from the viewpoint article and then wrap up with my thoughts:
However, the preponderance of available evidence from the fall school semester has been reassuring insofar as the type of rapid spread that was frequently observed in congregate living facilities or high-density worksites has not been reported in education settings in schools. Preventing transmission in school settings will require addressing and reducing levels of transmission in the surrounding communities through policies to interrupt transmission (eg, restrictions on indoor dining at restaurants). In addition, all recommended mitigation measures in schools must continue: requiring universal face mask use, increasing physical distance by dedensifying classrooms and common areas, using hybrid attendance models when needed to limit the total number of contacts and prevent crowding, increasing room air ventilation, and expanding screening testing to rapidly identify and isolate asymptomatic infected individuals. Staff and students should continue to have options for online education, particularly those at increased risk of severe illness or death if infected with SARS-CoV-2.
And the second paragraph:
Decisions made today can help ensure safe operation of schools and provide critical services to children and adolescents in the US. Some of these decisions may be difficult. They include a commitment to implement community-based policies that reduce transmission when SARS-CoV-2 incidence is high (eg, by restricting indoor dining at restaurants), and school-based policies to postpone school-related activities that can increase risk of in-school transmission (eg, indoor sports practice or competition). With 2 vaccines now being distributed under Emergency Use Authorizations and more vaccine options anticipated to be available in the coming months, there is much hope on the horizon for a safer environment for schools and school-related athletic activities during the 2021/22 school year. Committing today to policies that prevent SARS-CoV-2 transmission in communities and in schools will help ensure the future social and academic welfare of all students and their education.
So here are my thoughts. Yes, we can reopen K-12 schools safely but that depends on schools and the surrounding community committing to having a strong safety culture. Unfortunately, I think that there are too many school districts in Georgia and the surrounding communities that have NOT adopted a strong safety culture. I’ve seen the pictures of crowded hallways filled with maskless students. I’ve seen the pictures of full gymnasiums to watch a basketball game where no one in the building is wearing a mask.
We cannot live life as we did prior to the pandemic, not yet anyway. We cannot have our cake and eat it too. We need to prioritize the things that are most important. If it is vitally important for a local community to have indoor dining options (for the economic survival of the community, for example), then that’s not sustainable with safely offering face to face instruction. If indoor high contact sports are important, then perhaps it’s best for those children to attend school virtually, or postpone/cancel indoor sports until disease rates decline with the vaccination. All of this would be greatly helped by more centralized guidance and policies from the Georgia Department of Education and the Georgia Department of Public Health. Giving control over safety decisions to the local superintendents and school boards for a virus that doesn’t care about county borders or local politics and perceptions on disease risk makes no sense. It is passing the buck down the line because the people at the top don’t want to make a decision that will get them angry phone calls.
Let me be abundantly clear: being in the company of non-household contacts in an indoor setting without a mask and social distancing is an UNSAFE situation for any age group. That guidance has not changed. For my own children, they will not set foot inside of a school building, karate dojo, or other extracurricular activity where masks are not required and where social distancing is not observed until they are fully vaccinated against COVID-19.
References
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
WHCTF report repository: https://beta.healthdata.gov/browse
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
https://www.cdc.gov/mmwr/volumes/70/wr/mm7004e3.htm?s_cid=mm7004e3_w
https://jamanetwork.com/journals/jama/fullarticle/2775875
https://beta.healthdata.gov/National/COVID-19-Community-Profile-Report/gqxm-d9w9
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.