The Daily Digest, 14Oct2020
Georgia COVID-19 Updates

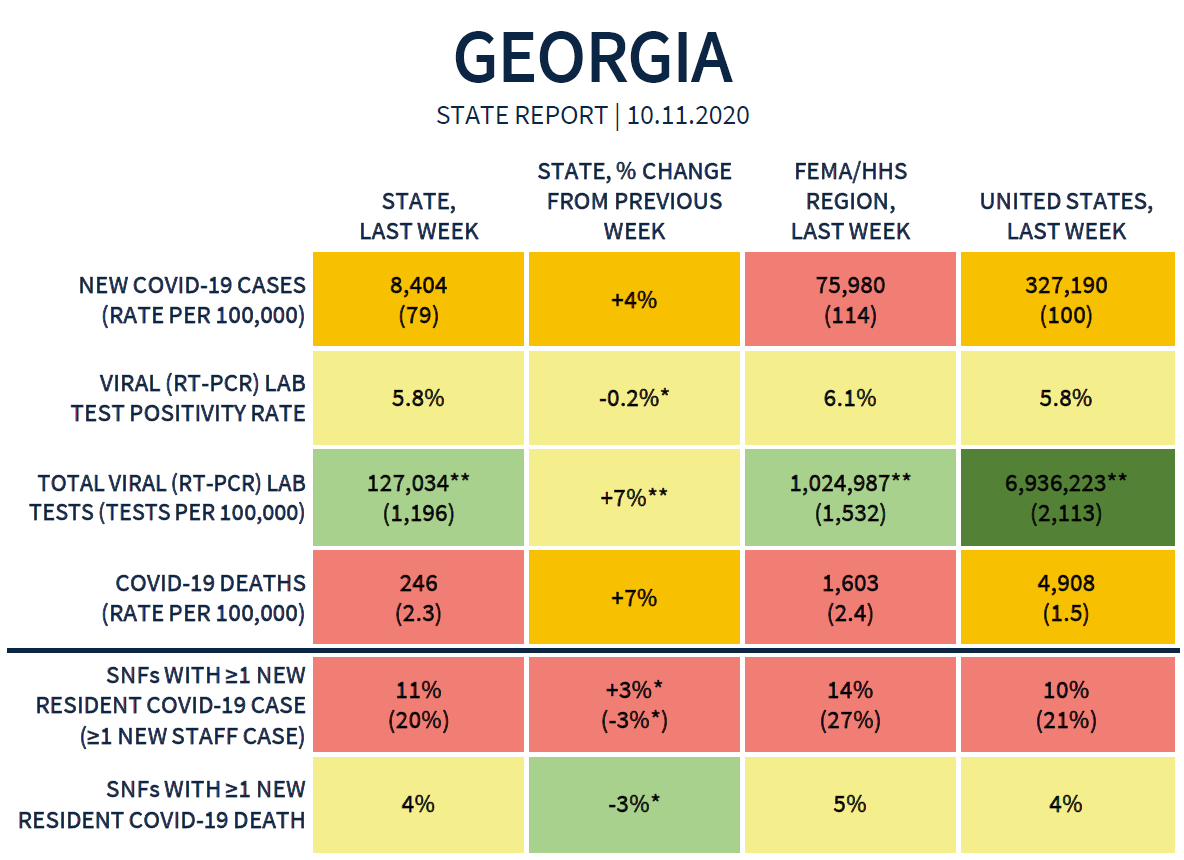
Good afternoon! Today we’ll be discussing the latest White House Coronavirus Task Force report (abbreviated as WHCTF from now on), the most recent county indicators report, and the latest daily numbers for Georgia in the COVID-19 pandemic. Let’s begin with a look at the summary table for Georgia from the WHCTF.
Testing
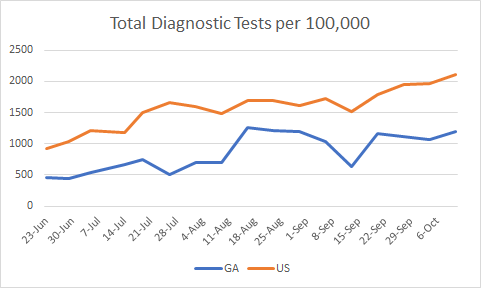
Georgia continues to lag behind the national testing rate per population and the disparity is growing. This is only for PCR based testing. This graph doesn’t include antigen testing for any state.
Our percent positive rate is holding steady while the national rate is surging. I would expect that next week we will be below the national average, not because we are doing better (though that would be great!) but because cases are surging in other parts of the country. Again, these data are based on PCR test results.

Today in Georgia, the state reported 23,760 new tests through Electronic Laboratory Reporting (ELR), a medium output day for us over the past month or so. Of those tests, 892 were positive, for 3.8%. Ordinarily that would be a great thing, but this was a low reporting day…of the new cases reported today, only 68.8% were reported through ELR. So we don’t have eyes on the remaining 31.2% of cases and how many tests (positive or negative) came from those laboratories or physician offices. It means that the 3.8% positive rate may not be a reliable assessment of positivity rate today. The state tends to have one day a week or so that is like this (see graph below).

Of the cases that were reported today, only 11.6% were reported prior to the 14-day window of uncertainty (normal is <20%) and this is independent of the ELR reporting problem. So the cases newly reported today are mostly recent.
Cases
The WHCTF collects case and death data from USAFacts, a nonprofit agency that gathers governmental data for all sorts of things including economic data, voting information, etc. The data for COVID is taken directly from each state’s daily report. So if a state includes probable cases in their case total, as the WHCTF recommends, then that is the number that USAFacts has gathered and that the WHCTF is using. Georgia does not do that. We’re going to come back to this throughout this section because it makes a very big difference in terms of how we compare to other states.
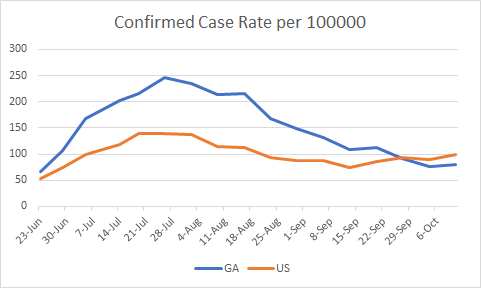
Georgia’s confirmed case rate per 100,000 is below the national average, but slightly higher than last week. Keep in mind that most states are including antigen test-identified cases in their case total, whereas Georgia is not.
The number of counties on the WHCTF list of counties of concern continues to decline. These are based on case rate and the impact of antigen-based testing is not accounted for in these graphs or determinations by the WHCTF.

A new addition to the WHCTF reports is a national picture for cases, testing and deaths, with rankings of the states for each (see below). For a state to be in the red category for cases, they need to have a case rate of >101/100,000 in the most recent week. Using PCR testing only, Georgia is in the orange category, and ranked #33 in the nation. If last week’s total cases from WHCTF (8404) is combined with the antigen test-identified cases from the DPH County Indicators report (2131), then our case rate per 100,000 is 106.1. We belong in the red zone if probable cases are included in our case total, as they are for most other states in the US.

Of course, it is very disheartening to see very little green left in this map that shows new case rate per 100,000 across the US, especially as we head into influenza season. As a country, we have not done the work to prepare for winter and I think we should all brace for some grim months to come.
The map provided below shows the way that inclusion of Georgia’s most recent probable cases (most are based on rapid antigen testing) increases the total case count for each county. Click on the image below to see a “live” version of the image where you can click or hover over your county to see your local percent increase. Knowing this increase helps you to have a better sense of how intense disease is in your area. The more blue the county, the less probable cases are playing a role. The redder, the more intense the effect. Unlike other maps for Georgia data, the white counties don’t indicate a lack of data, but rather that they are at the midpoint of the spectrum for the effect of probable case inclusion in the county total.

From the DPH County Indicators report, here are the counties that are on their radar as counties of concern. If your county is on this list, you need to be taking precautions and limiting your exposures as much as possible.

Today in Georgia, there were 1297 newly reported cases, bringing the state total to 334,601. Forty nine percent of the cases came from nonrural counties outside of the Atlanta metro. Thirty five percent came from the Atlanta suburbs and 27% came from rural counties. A significant backlog was cleared from the “unknown” county class.
Hospitalizations
Something very strange in the latest WHCTF report is that they report a jump in confirmed case admissions. This is a big departure from the data we have been provided from the state. It’s possible this is a typo in the WHCTF report, but the WHCTF does not have a website, much less a phone number for me to call for clarification.

From today’s numbers from Georgia DPH, there are 156 new hospital admissions for COVID-19 and 23 new admissions to the ICU. The current number of patients hospitalized stands at 1325, slightly below yesterday’s number but higher than where we were a week ago. Adult ventilators are in use at a rate of 29%, consistent with pre-summer surge levels. There are three hospital regions using >90% of their ICU beds at present: regions E (90%), H (95%) and N (93%).
Deaths
The Georgia death rate remains higher than the national average. They note the same increase in the most recent week than the week that preceded it as I did on Sunday. The national death rate is declining for now. But with cases surging in parts of the country, and deaths being a lagging consequence of case surges, we should expect the national rate to increase in the coming weeks.

There were 16 deaths newly reported today in Georgia. Nine of them came from rural counties and 4 came from the Atlanta counties. The updated state total is 7470.
Here are some highlighted recommendations from the WHCTF report. You can read the full list here.
“Increase surveillance for silent community spread. Use the Abbott BinaxNOW or other antigen tests as weekly repeat surveillance in critical populations to monitor degree of silent (asymptomatic) community spread among K-12 teachers; staff working at nursing homes, assisted living, and other congregate living settings; prison staff; and first responders. All antigen positive results must be reported with both the number of positive results and total tests conducted; positives must be reported as COVID cases.”
They go on to say that “repeat testing of individuals as surveillance with confirmation of all positives with nucleic acid testing is the optimal use of antigen tests.” Meanwhile, here’s what CDC has to say about the rapid antigen test:
“The clinical performance of rapid antigen diagnostic tests largely depends on the circumstances in which they are used. Rapid antigen tests perform best when the person is tested in the early stages of infection with SARS-CoV-2 when viral load is generally highest. They also may be informative in diagnostic testing situations in which the person has a known exposure to a confirmed case of COVID-19. Rapid antigen tests can be used for screening testing in high-risk congregate settings in which repeat testing could quickly identify persons with a SARS-CoV-2 infection to inform infection prevention and control measures, thus preventing transmission. In this case, there may be value in providing immediate results with antigen tests even though they may have lower sensitivity than RT-PCR tests, especially in settings where a rapid turnaround time is required. See FDA’s FAQs on screening asymptomatic individuals and use of antigen tests in high risk congregate settings.
There are limited data to guide the use of rapid antigen tests as screening tests on asymptomatic persons to detect or exclude COVID-19, or to determine whether a previously confirmed case is still infectious.”
In addition, here’s a table that summarizes how well negative and positive tests can be trusted in different situations.

The pretest probability is probably on the higher end if a person has a known exposure to a confirmed case, whether part of an outbreak investigation or due to the nature of their work (for example, healthcare workers). In this case, you can trust a positive result, but there’s also a risk of false negatives meaning, a person is actually positive. The pretest probability might be low if a person isn’t displaying symptoms and doesn’t have a known link to a confirmed case. In that case, you might be more likely to see false positives (where a person is actually negative), but you can better trust a negative result. Depending on which situation you’re in, the CDC recommends getting a confirmatory PCR test - if you’re asymptomatic with no link to a case and you test positive; and if you’ve had a high risk exposure, maybe display symptoms but test negative.
It seems like there’s a disagreement between CDC and the WHCTF or perhaps more nuance to when the test is best applied. The CDC indicates that the test is best used for those who are symptomatic or who have a higher likelihood of testing positive. The WHCTF is recommending that the test be used to identify asymptomatic individuals. The state of Georgia has indicated they plan to deploy these tests to “schools, colleges and universities, among first responders and other critical areas of need in communities statewide.” These are the settings where disease is perhaps more likely to be and might be in that high probability zone. But it does seem that CDC and the WHCTF don’t understand the rapid antigen test in the same way. The CDC approach seems to be the more conservative strategy of the two. And when lives are on the line, we want to be as careful as possible. Regardless, the WHCTF is continuing to call for Georgia to include cases identified through rapid antigen testing to be counted in the state’s case total and we are not, so far.
The WHCTF also warns that they are seeing community spread initiated by social gatherings with friends and family. It’s important to remember that although you may love a member of your family (who doesn’t live with you) and trust them with just about anything, you are buying the disease risk that they have taken in their daily life before your encounter. So all of their exposures are now your exposures. And those exposures accumulate and increase your risk of getting sick. No one deliberately brings a disease to a family gathering. But the virus doesn’t care about love or friendship and those sentiments are not a shield against contracting the disease. If meeting with family or friends is a priority to you, then you need to minimize your exposures in other areas and take fewer risks. This is the way that quarantine pods function.
Lastly, my latest episode of Public Health for the People was released today. It has to do with voting during a pandemic.
References
https://www.documentcloud.org/documents/7229961-Georgia-10-11-20.html
https://countyindicatororeport.s3.amazonaws.com/county_indicator_report_201012.html
https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.