The Daily Digest, 11Nov2020
Georgia COVID-19 Updates

First, from my family to yours I want to wish a happy Veterans Day to all of my readers who have served or who currently serve in the US military. It’s an honor to be a part of this family with you and I’m deeply appreciative of your service to our nation.
Today we’ll be talking about the latest White House Coronavirus Task Force (WHCTF) report and the latest numbers for Georgia. Here’s the summary table from the most recent report.

Testing
There seems to be a bit of data correction that is happening in between the reports from the WHCTF. Because the summary table notes that the positive rate for Georgia increased by 0.2%, but this week’s reported rate is 7.4% compared to 7.5% in last week’s report. Based on what the WHCTF is giving us on a weekly basis, here’s how test rate per population and positive rate compare to the US over time. Keep in mind that both graphs are only considering the PCR test and this does not factor in the antigen cases.

The test rate per 100,000 for Georgia has always been below the national average but the gap has widened over time. To be fair, it’s possible that Georgia is doing better with testing thanks to the arrival of the antigen test, but this graph doesn’t capture that, nor does Georgia report those data. But based on PCR alone, we are testing at a rate that is 50% less than the national average.

The positivity rate has increased nationally and now surpasses the Georgia rate, however our rate is very close to the national average right now. Remember, the positive rate is often considered alongside the case rate. The case rate per 100,000 tells you how intense disease is for a given area. The positive rate tells you the degree to which that case rate might be an under count of the situation. The greater the positive rate above 5%, the more likely we aren’t testing enough and are missing cases.
Today in Georgia, there were 13,522 new PCR results reported through Electronic Laboratory Reporting (ELR) and of those 8.7% were positive. Seventy one percent of the net increase in PCR cases today were reported through ELR so it’s a bit of a low data collection day, but not as drastic as we’ve seen in the past. Using a recent example (the election) we all learned that you can’t call the election for a given candidate in a county when only 70% of precincts are reporting. When we don’t have eyes on the data that support 29% of the PCR cases that were reported today, then we don’t have a clear view on the situation. Therefore, the 8.7% positive rate for today’s data might not be the best estimate of our true positivity rate. This is one of several reasons why it’s important to pay attention to trends, rather than single day occurrences. We don’t have data on the number of antigen tests performed or a positive rate for that test. As the test gains in popularity (for example, it identified 27% of the net increase in total cases today) then the positive rate for PCR alone becomes less significant. Ideally, we need the positive rate for both tests, but that’s problematic with a point-of-care test like the antigen test.
Cases
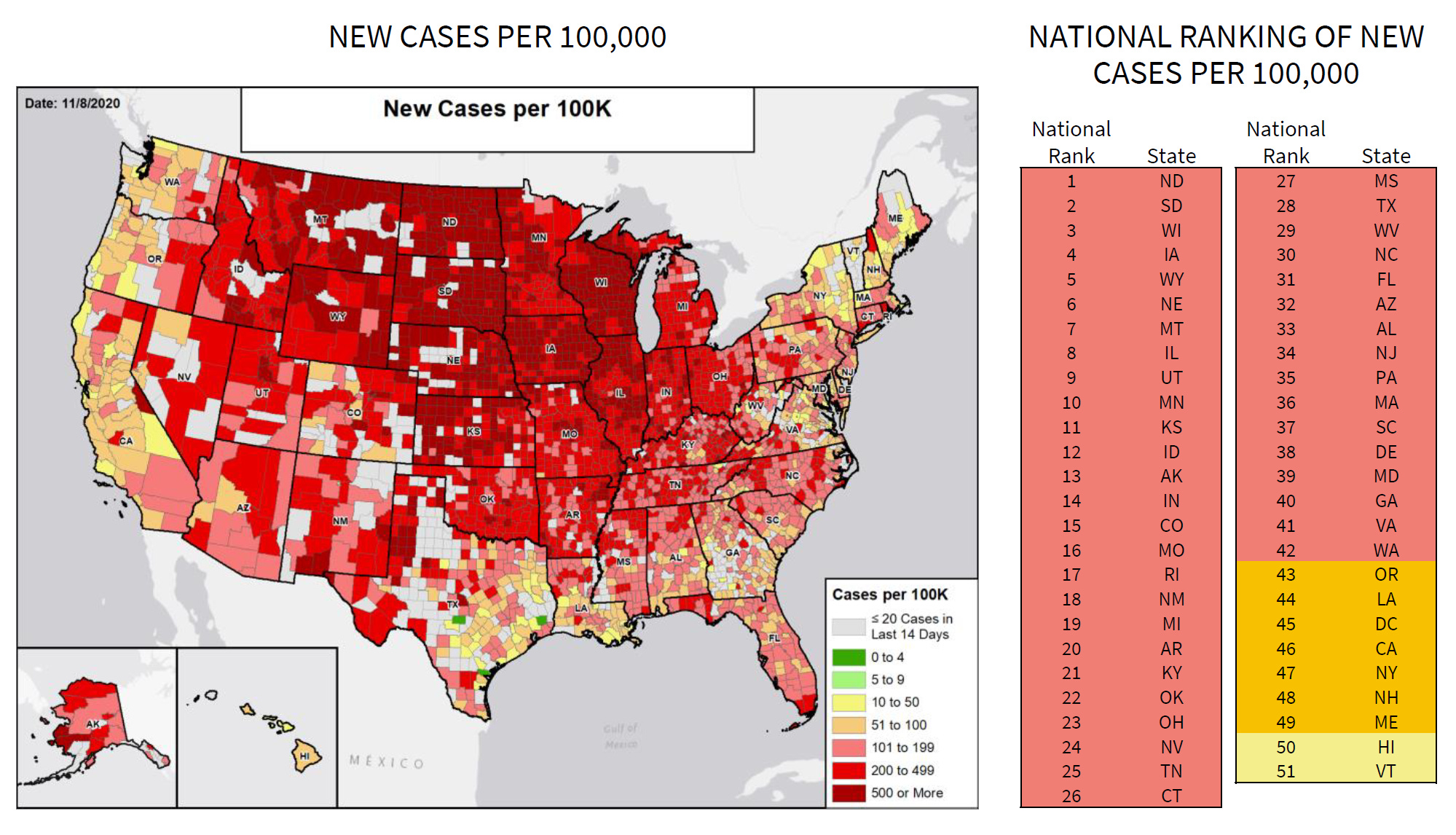
The biggest piece of news out of this week’s report is that Georgia is back in the red zone and we are ranked #40 in the nation. There are 42 states in the red zone this week. It is important to understand that this surge is different than the previous ones that the US has experienced. In the past, the surges were regionally focused - in the northeast in the spring and in the south during the summer. When they’re regionally focused like that, it’s possible to send in reinforcements of supplies and personnel. When the surge is taking place nationwide, it might mean that we’re all on our own more so than in previous surges. So we are really not in a good spot as a nation right now. We really need for people to take this seriously.
Here’s how the case rate per 100,000 looks for Georgia compared to the US. Again, remember that Georgia is only reporting PCR-identified cases to USA Facts, the repository of information that is used for the WHCTF reports.

You can see that both the national and state case rate is increasing, with the national rate increasing more sharply than the rate for Georgia. The next graph shows how the number of counties on their list of counties of concern has varied over time. The number of counties in the red, orange or yellow zones are color coded in that same scheme on the graph. The total number of counties on the list (red + orange + yellow) is represented by the black line.

The total number of counties on this list has been increasing steadily since mid-October. From the recommendations of the WHCTF (see recommendations section at the end of this post), they indicate that counties in the red and orange zones should be doing proactive testing of 18-40 year olds, where asymptomatic carriage of disease is more common. This means going beyond just testing those who are curious or who have symptoms. It means actively looking for the disease at the settings where we expect to find it, regardless of their symptoms.
Today there was a net increase of 2242 new cases compared to yesterday’s total (PCR = 1640, antigen = 602). The updated statewide total is 413,894 cases (PCR = 377,694, antigen = 36,200). The greatest contributor to cases today was nonrural counties (38% of cases). Atlanta suburb counties and rural counties were equivalent at ~24% each.
Hospitalizations
In the most recent week’s WHCTF report we’ve seen two interesting developments with regard to hospitalizations. First, let’s look at the graph that shows how the WHCTF has reported hospital admissions (confirmed and suspected COVID-19 cases) over time. The gray line corresponds to the right y-axis and depicts how many Georgia hospitals are reporting in to the system.

Reporting has held steady for the past month (a good thing!). This week’s report indicates a decrease in the number of hospital admissions, but the summary page discusses that hospital admissions have plateaued. That’s consistent with what I’ve reported earlier this week on Sunday.
Another interesting thing to note is that the WHCTF specifically calls out Georgia’s deficiency in PPE supplies for Georgia hospitals in the recommendations section. In the image below, you can see how well supplied our hospitals are for PPE this week compared to last week.

Last week, roughly 90% of Georgia hospitals had only 0-3 days worth of PPE on hand - not a good spot to be in if cases are increasing and we know that hospitalizations are a lagging indicator. This week, we saw that now ~50% of Georgia hospitals have only 0-3 days worth of PPE on hand. So that’s a big improvement in a week’s time. But we would really rather see this number go lower. The last thing we need is for our healthcare workers to run out of PPE.
Today there are some concerning things regarding hospitalizations for Georgia. There are currently 1620 patients hospitalized for COVID-19 disease. We haven’t been above 1600 since 08Sep. There were 175 patients newly admitted today and 33 were admitted to the ICU. Statewide, 10.2% of all hospitalized patients are there for COVID-19 treatment and management with an additional 2.4% of patients suspected of having COVID-19 disease but pending laboratory results. The part of the state with the greatest hospitalization rate right now is hospital region A in northwest Georgia (23.2%). That is also where many of our red counties are clustered right now by both the WHCTF threshold and the Harvard Global Health Institute threshold. This might seem obvious, but sometimes I think people forget - hospitalizations are the result of cases. The fewer cases we have, the fewer hospitalizations. So all regions should be doing what they can to limit the number of cases in their community.

Deaths
The graph below shows how the WHCTF has reported the Georgia death rate compared to the US average over time. You can see that Georgia has come a long way down following the summer surge. This week our death rate matches the national average and this is because death rate is increasing for the US while the Georgia rate is holding steady. Hospitalizations and deaths are lagging indicators that follow case increases. The best way to keep hospitalizations and deaths down is to keep cases from happening in the first place.

Georgia reported a net increase of 69 deaths today and this is a higher number for us than we’ve seen in recent weeks. In fact, the last time we had a number this high was 23Sep. Thirty two (46%) of today’s deaths came from rural counties and 17 (25%) came from nonrural counties. The updated total number of deaths for Georgia is 8333.
Recommendations
The recommendations this week are really specific compared to previous weeks where it seemed like things were really vague. I’ve highlighted some notable pieces of information in the recommendations below. But a common theme I noticed is that the WHCTF doesn’t think Georgia is doing enough testing, or is not conducting their testing in the right way. They are really emphasizing that Georgia needs to do proactive surveillance testing, specifically among 18-40 year olds, in red and orange counties. The 18-40 year old thing is important because that age group is the main source of our cases and also the age group that might be more likely to experience mild, if any, symptoms with coronavirus. So testing and isolating infected individuals in this age group will do a lot to prevent spread to older, more vulnerable populations. Georgia’s strategy to date has been very reactionary - testing those who are symptomatic or curious and offering testing to close contacts identified during contact tracing. The WHCTF is advocating that Georgia add this proactive testing effort to its overall strategy. What might this look like? It means looking for disease where we expect to find it (i.e. red and orange counties, places where people gather, etc), testing a subset of a given population regardless of their symptoms. If we can sideline as much of the virus as we can by finding the asymptomatic cases and isolating them, the virus has fewer opportunities to spread to others.

They also recommend avoiding social gatherings outside of ones household and have some guidance on the upcoming Thanksgiving holiday. I spoke to a business organization this morning and they had a question about how Thanksgiving should look this year. I heard, “Thanksgiving just isn’t the same if Grandma isn’t there.” That’s correct, a lot of things in 2020 just aren’t the same and Thanksgiving is no exception. No one in public health enjoys ruining the holidays with this guidance. We all have families too, many of whom we haven’t seen since early 2020. I know many of us crave the idea of getting back to normal but we don’t have the conditions on the ground to do that yet. I think we all need to consider whether it’s more important to have Grandma at Thanksgiving or to have her for the years to come, for new grandbabies, graduations and birthdays, weddings and future holidays. I really recommend keeping your gathering as small as possible, ideally just the people who live with you or those in your quarantine pod if you have one. If you are planning to gather beyond that, prioritize having your gathering outside (Georgia weather is often beautiful for Thanksgiving) and keep the celebrations distant and brief. Remember, it’s not enough to wear a mask but then sit shoulder to shoulder with others around the dinner table. These risk mitigation strategies do not stand alone - they need to be used in combination.
That’s it for today. Be safe and be well!
References
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
https://usafacts.org/visualizations/coronavirus-covid-19-spread-map/
https://amberschmidtkephd.substack.com/p/the-week-in-review-02-08nov
https://drive.google.com/file/d/1R4vaeOMJkjMX2QQknT0DbQYTtlAJNOeH/view?usp=sharing
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.