The Daily Digest, 09Oct2020
Georgia COVID-19 Updates

Last month, the CDC released guidance on Halloween celebrations. I’ve put together a chart of their suggestions for low-, moderate- and high-risk activities that families can consider this year in the context of COVID-19.

One thing you’ll notice is they really don’t want you spending time inside with people who don’t live in your home. Every family will have to weigh their own risks. The safest options are in the low-risk column. In the moderate risk column, they focus a lot on outdoor activities and I should add that if an event is likely to have screaming or shouting (i.e. haunted forest, Halloween movie, etc), then you need more than 6 feet of distance between you and others. I know many will be disappointed to know that they consider both traditional trick or treat and trunk or treat events to be high risk. Both of those are outdoor or semi-outdoor events and you’d think that would be okay. But there can be some crowding and congestion during these events that I think CDC wants us to avoid. There are creative ways to still do this with candy chutes and I’ve even seen a zipline delivery method on TV. For my house, we’re going to use a candy chute. I think it will honestly be kind of fun. I’ve heard memes and people asking if getting take out or curbside pickup is okay, then why isn’t trick or treating okay? I think the difference is the scale. On Halloween there are throngs of people and close contact exposures. It’s the difference between a handful of families in a neighborhood getting takeout at a restaurant versus every kid in the neighborhood (and their parents) coming to each door for that close contact encounter. It’s really not comparable.
While I appreciate the CDC coming up with this list, scavenger hunt lists don’t just make themselves. I made one for my neighborhood and thought I’d share if anyone else needs it. If you’d like the original file so you can add/subtract things, please email me at amberschmidtke.phd@gmail.com.

Testing
Today there were 29,508 new PCR test results (the gold standard) reported. Of these, 4.9% were positive. We’ve been at or below 5% for the past two days now, a great development. And this 4.9% is a reliable number since Electronic Laboratory Reporting accounted for 89% of today’s total increase in cases.
Haley, the Open Records Request maven, got more data on the PCR, antigen, and antibody (serology) tests from the Department of Public Health.
In the first graph below, the bars represent total tests reported through ELR for each test type (right y-axis). The lines represent percent positive rate (left y-axis). The color coding is the same. So red = antibody test, blue = PCR test, green = antigen test. You can see all the data DPH sent over here.

The percent positive rate between PCR and antigen tests (blue and green, respectively) is pretty similar and both are trending down. Another neat thing we learned from the Open Records Request is the time delay between specimen collection and when the result was reported through ELR. In the next two graphs, the bars correspond to the right y-axis and show you total test output for that day. The lines (left y-axis) tell you the number of days. In red we are looking at the mean (also knows as the average). The green line is the median, or the middle-most number, which is less susceptible to outliers in data.

The median range for this time delay for PCR is 2-5 days since the start of the pandemic. The mean range has varied between 2-9 days.
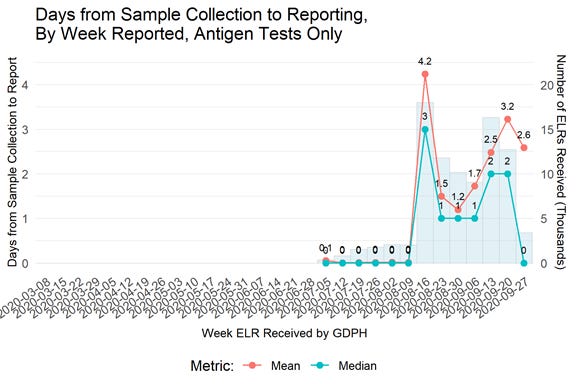
By comparison, the median range for the antigen test is 0-3 days and the mean range is 1.2-4.2 days. This is not surprising, since this test does not require specimen processing and shipment, and the results are ready in 20 minutes.
We also got a look at who the most prolific reporters are through ELR. This is likely not an exhaustive list. The criteria they set was labs that were reporting >1500 total PCR tests, including at least 20 positive antigen (Ag) and PCR tests, respectively. The First graph shows tests in the thousands. Percent positive is represented by the dots. So the big three are Archibold Medical Center, Bio Reference Laboratories, and South Georgia Medical Center. Both Archibold (Region K) and South Georgia Medical Center (Region L) did thousands of antigen tests.

The next tier of labs are represented on the graph below with a really compressed y-axis. I can’t adjust this; it’s how DPH gave it to us as a flat image. The y-axis for ELR reports is in the hundreds.
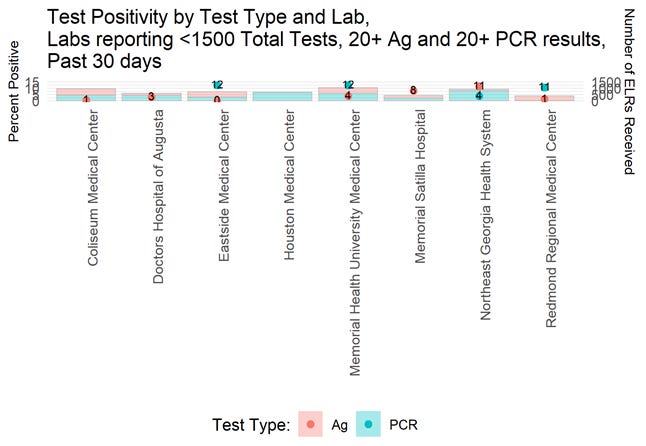
Together, this helps us to see a bit better where the antigen tests have been prioritized and that is for South Georgia in hospital regions K and L, according to the data that were provided.
Cases
There was a net increase of 1625 new cases reported today, bringing the statewide total to 329,032. Keep in mind, this total only includes PCR test-identified cases. There are at least 23,000 more identified by antigen testing as of Monday’s county indicators report (these data are only updated weekly).
Something interesting is going on with the 7-day case rate per 100,000 by date of report. Atlanta counties have climbed, overtaking the statewide average.

The increase seems to be attributed to Fulton county, specifically, that has seen an increase in case reports, and particularly among 18-22 year olds (read: college-aged adults) in recent weeks. But cases have been steadily rising among 5-17 year olds for the past 10 days too.

However, this might be due to delayed reporting, not necessarily recent illness, if we compare the graphs for cases by date of symptom onset versus report. Note that there’s an increase in the graph on the left compared to the graph on the right. However, the 7-day average for Fulton county does appear to be increasing through the 14-day window of uncertainty for date of onset. There may be an increase lurking in that 14-day window of uncertainty, so I would just advise Atlanta residents to just be sure to be vigilant.

I wanted to take time to explain this, since so many different organizations (i.e. New York Times, COVID Tracking Project, Harvard Global Health Institute, and some of the reports from DPH) use date of report rather than date of symptom onset when comparing counties, states, etc.
Today we got the latest school-aged surveillance data report. Here’s how school-associated clusters have varied over time. DPH counts K-12 and college/university settings together. They don’t provide actual numbers, but it looks like there’s just under half as many clusters this week compared to last week. Here’s how they define a cluster: Laboratory-confirmed COVID-19 in two or more people (students or staff) with symptom onset/collection dates within a 14 day period who are epidemiologically linked, do not share a household, and were not identified as close contacts of each other in another setting during standard case investigation or contact tracing.

Hospitalizations
There were 124 COVID-19 hospital admissions newly reported today and 29 ICU admissions. Thirty percent of the adult ventilators are in use (for all reasons, not just COVID-19) and this is consistent with where we were prior to the summer surge. Current hospitalizations dropped by 37 patients today and that’s certainly something that I hope will continue.
In the school-aged surveillance report, there’s an increase in COVID-19 hospitalizations for 18-22 year olds in the most recent week. These are based on date of report, so it’s possible that the prior week’s sharp decrease was an anomaly of poor reporting that week. There’s also an increase among 14-17 year olds, but that seems to be part of a trend for them where there are spikes in the data every couple weeks.

You may not know, unless you’re a data nerd, that DPH recently expanded the data offerings in the “download the data” section at the top of the daily report. Among the new files is more information on cases, deaths and hospitalizations for healthcare workers. To date, there have been 19,928 cases among healthcare workers and 99 of those were reported today alone, 429 in the last 7 days. There have been 1277 hospitalizations among healthcare workers (6.4% of cases). Lastly, there have been 134 deaths among healthcare workers, or 0.7% of the cases identified in this population. It’s important to remember that all of these are likely to be under counts, since DPH does not get occupation information for every case. This is just what we know.
There are just two hospital regions using >90% of their ICU beds, regions B (northeast Georgia) and N (northwest Atlanta metro).
Deaths
There were 54 newly reported deaths today, which is the highest we’ve seen in 14 days. These deaths bring the statewide total to 7348. Forty two percent of the deaths came from rural counties, and another 31% came from nonrural counties outside of the Atlanta metro. Below, you can see the updated 7-day death rate per 100,000 graph. The gap between rural counties and the statewide average is widening.

In fact, the death rate in rural Georgia is so intense that if it were its own state, it would have the 3rd highest death rate in the nation over the past 7 days, behind North Dakota and Guam. Compared to global death rates, rural Georgia would be in third place, right behind Kosovo and Argentina. Meanwhile, the United States is ranked 28th in the world and Georgia (as a whole) is ranked #13 in the nation.

On that less than happy note, that’s it for today. Have a safe, socially distanced weekend. I’ll be back on Sunday with the week in review.
References
https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/holidays.html
https://drive.google.com/file/d/1y90VfWj1NBq9a-3G6-Z3LKg55-K_M6lr/view?usp=sharing
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
https://www.nytimes.com/interactive/2020/us/coronavirus-us-cases.html
https://www.nytimes.com/interactive/2020/world/coronavirus-maps.html
https://epidemiologyschoolreport.s3.amazonaws.com/SchoolAgeSurveillance928.html#introduction