The Daily Digest, 05Feb2021
Georgia COVID-19 Updates

Public Health Advocacy
The Georgia Senate Appropriations Committee has approved $11.1M in new funding for the Department of Public Health, in addition to the new funds passed by the Georgia House. Some of these funds are dedicated to new administrative positions - a senior programmer and a financial manager. The rest is listed in the Epidemiology section and it appears to be additional cushion money in case replacing the GRITS vaccine tracking system is more costly than anticipated. You can see the proposed budget in full here.

All in all, the funding from the House and Senate Appropriations Committees add up to $43.1M in additional funding for DPH through June 2021 compared to the Governor’s request. It will next go to a full Senate vote.
These are important improvements and I’m grateful for the work that legislators have done to find money for public health. It is my hope that this is just a down payment on a sustained commitment to improving public health in Georgia. To that end, we need to start our advocacy work anew, for the FY22 budget, beginning with the House Subcommittee on Health Appropriations (contact info gathered here) and the representative for your area as well. If you’ll recall, this is the one where the Governor proposed no new funding for DPH during the middle of a pandemic response that has identified serious deficiencies in the state’s public health infrastructure.
Vaccine Update
The Vaccine Adverse Event Reporting System (VAERS) is an early warning system of sorts to see if there’s something wrong with the vaccines. Anyone can report to this system, including physicians, vaccine recipients and their caregivers. The reports are unverified and as a result, it’s not really possible to make conclusions about association with any vaccine without further investigation. You can see part of the VAERS disclaimer below.

In fact, years ago, an anesthesiologist tried to highlight how unreliable this system was by reporting that following his annual flu vaccine, he turned into The Hulk. His report was accepted by VAERS and showed up in the results. Eventually, CDC saw it for what it was and asked his permission to remove it from the database. If not for that, however, turning into The Hulk would still be listed as one of the adverse events following influenza vaccinations on the site.
I bring this story up to remind you all that while I periodically keep an eye on this database, we all need to take its findings with not just a grain of salt, but a generous teaspoon of salt. It represents the very worst case scenario because it is filled with redundancies, coincidences, and outright fabrications. Unfortunately, it is a favored resource for anti-vaccine groups to highlight because the CDC association gives it an air of legitimacy and then they cherry pick the things they want in order to convince people that vaccines are not safe.
As of today, CDC is tracking that 35.2 million doses of the COVID-19 vaccines have been administered. According to the VAERS database, there have been 520 entries (people) for severe events that required an emergency department visit. The top ten symptoms are ranked below. Keep in mind that a person can have more than one symptom so there is a mismatch between the symptoms reported (n = 4469) and the people reported (n = 520).

Some of these terms will be unfamiliar. Dyspnoea = shortness of breath, pyrexia = fever, paraesthesia = tingling sensation, hypoaesthesia = reduced sensation. Note that SARS-CoV-2 test negative is listed as one of the “symptoms.” That’s a laboratory finding. So hopefully that reinforces the idea that some of these symptom entries are redundant or not applicable. Even still, even if all of these 520 people had an event that was truly linked to the vaccine following investigation by a medical team, that’s still a rate of 0.0015% of all doses administered. The vaccine remains very safe so far.
A safety tracking resource that CDC is using following the COVID-19 vaccines is called v-safe. This is an app in which vaccine recipients self-report their symptoms following vaccination. Clinically important side effects get reported for investigation in conjunction with the CDC and the FDA. Some of the findings were reported at the most recent ACIP meeting. Among the interesting findings is that there have been at least 15,000 pregnancies reported to v-safe. That doesn’t mean that the vaccine made women pregnant. Rather, it means that pregnant women took the vaccine and self-reported their pregnancy so that the government could keep a special eye on this population for side effects and pregnancy outcomes. That’s pretty important considering that the clinical trials for these vaccines didn’t include pregnant women.
But the bulk of the v-safe findings had to do with reactogenicity. This is what we expect your immune system to do following a vaccination. This is different than an adverse event which is a more serious side effect above what was commonly found during the clinical trials. They offered this summary table below comparing the two available vaccines and the differences between dose 1 and dose 2. These data were gathered at a time that it was too early to collect data on dose 2 reactogenicity for the Moderna vaccine.
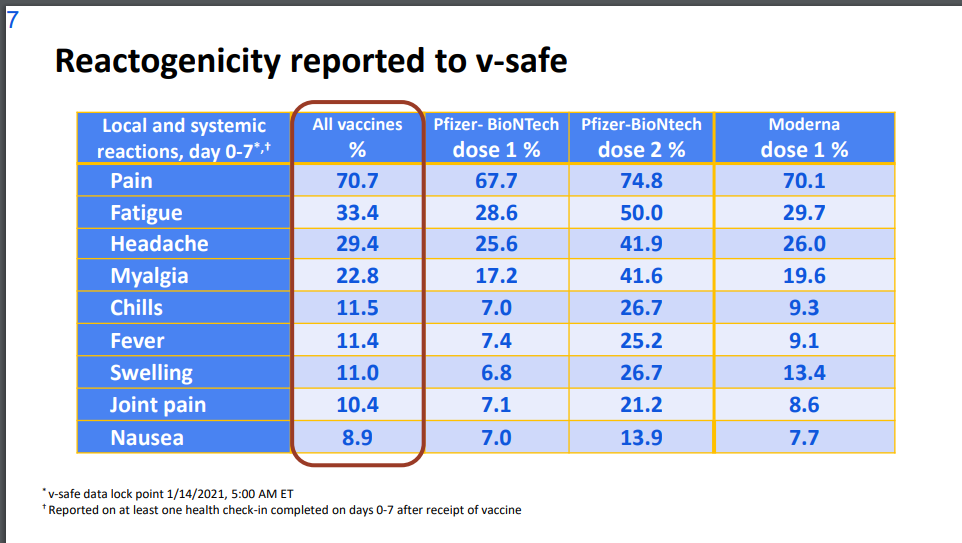
Start with the symptoms noted. You’ll see that they are a lot of the same top symptoms reported to VAERS. So, the top symptoms in the VAERS database were *expected* and wouldn’t really be considered “adverse events.” But in the v-safe data we see that in the first week, there are some symptoms that vaccine recipients should expect, regardless of which vaccine they received. Many of these symptoms are the cardinal signs of inflammation - proof that your immune system is reacting to something it doesn’t recognize. So as uncomfortable as they are, it’s a reassuring thing to see these symptoms because it means your immune system is doing what we want it to do and devoting energy (see the fatigue symptom) toward that effort. Next, move to the middle two columns. You’ll notice that there is an increase in reactogenicity for all symptoms for the second dose of the Pfizer vaccine. This is not a reason to skip the second dose, but maybe try not to make important plans for the following day. In the last column we can see the data for the Moderna vaccine, first dose. The percentage of patients reporting the top symptoms is somewhere between the dose 1 and dose 2 data for Pfizer. It’s possible that a similar trend will be noted with the second dose of the Moderna vaccine being more intense. I don’t bring this up to frighten anyone, again these are expected symptoms. But I want to make sure you know what to expect if/when you have these symptoms after immunization. These are normal, will probably only last a day or two, and can most likely be well-managed with over the counter pain medications. In the end, I think this is a small price to pay for immunity from COVID-19.
The exciting piece of news is that the FDA’s vaccine advisory panel will meet to discuss the Emergency Use Authorization application for the Johnson and Johnson vaccine on February 26th. This will be our first chance to see the clinical data for this vaccine.
Testing
Georgia reported 35,415 new PCR test results today, a mid-range day for the state. Of those tests, 10.8% were positive. As of today, we’re about 100,000 behind last week’s testing output total and I doubt we’re going to make that up tomorrow and Sunday. So we are likely looking at a decrease in test output this week. The question is by how much. It’s possible that some of the decrease is due to the shift in personnel from test collection sites to vaccination sites. And I’m worried about the more transmissible variant that is likely to be widespread in Georgia. Seeing testing output decrease means we might not see the impact of the more transmissible variant until we are overwhelmed by it. However, the percent positive rate continues to decrease even as test output decreases. That would suggest that we aren’t increasing the number of cases we’re missing due to lower testing. So for now, at least, we are in okay shape.
From the school-aged surveillance data report for 05Feb2021, the DPH includes test positivity data for children and college-aged adults. The test positivity rate has leveled off, but remains high for all age groups. It is highest among K-12 aged children, at 18.2%. The goal is to be at or below 5% on a sustained basis. So we are likely missing a lot of cases for 5 - 17 year olds.

Cases
Today there was a net increase of 4842 newly reported cases (3527 by PCR and 1315 by antigen test). Of today’s newly reported cases, 36% came from nonrural counties outside of the Atlanta metro, 30% came from the Atlanta suburbs and 21% came from rural counties. The 7-day case rate for the state has dropped 55% since the January peak, however we still have a lot of disease circulating in the community. The current case rate remains 19% higher than the height of the summer surge and we are nowhere near our pre-winter surge level.

Another way to look at our progress is by looking at maps side by side that show the 14-day case rate per 100,000 that includes both PCR and antigen identified cases from about a month ago and today. These maps are formatted the same way as the Georgia DPH maps in terms of the color break points. The only difference is the inclusion of antigen cases.

The winter surge peaked on 10Jan. In the 04Jan map on the left, there were 84 counties that surpassed the highest color tier. In today’s map on the right, there are only 16 such counties. Intensity is clustered in north Georgia, and what looks like hospital regions E and G. You can click on the image above to see the live image of the most recent map, so that you can see what’s happening in your county.
Hospitalizations
Today Georgia reported 232 new COVID-19 hospital admissions and 44 new admissions to the ICU. These are high numbers but not the highest we’ve seen during the winter surge. Unfortunately, the patient census and hospital capacity dashboards are undergoing critical maintenance and are not updating, for the second time this week. I can tell you that ever since the state’s COVID-19 data task force was stood down in August, the people who developed the dashboards have been reassigned to their regular job duties and no one is curating these dashboards or maintaining them. They only know there’s a problem when someone (usually me) let’s them know and then their instructions are only to keep the dashboards alive, but not to do any proactive maintenance to make them run more efficiently. It is yet another example of the lack of priority the state has dedicated to data fidelity and informing the public during the pandemic.
We do have the data that Georgia hospitals report to the federal government in the meantime. It’s more cumbersome to read than the dashboards however, and it’s not organized into hospital regions. It tells us that 88.6% of Georgia’s staffed ICU beds are full and 37.3% of the ICU beds in use are held by COVID-19 patients. They report 4072 patients currently hospitalized for COVID-19, 3996 of which are adults. There are 76 pediatric patients hospitalized (<- this is more information than the state provides to the public).
ER visits for children and young adults with COVID-19 syndrome is declining for most age groups. But they remain at a high level for children 0 - 10.

Deaths
There were 98 newly reported confirmed deaths today. This is a high number but less than we’ve seen recently. So I’ll take that good news. Of today’s deaths, the largest contribution came from nonrural counties outside of the Atlanta metro (32.6%), followed by rural counties (27.6%), Atlanta suburbs (18.4%) and Atlanta counties (Fulton and DeKalb, 16.3%). The graph below shows you how the 7-day death rate, adjusted for population, has trended over time for each of the county types in Georgia. We remain at a high level, but the death rate is highest for rural counties. That’s consistent with the trends for every surge so far.

Schools
I just wanted to take a moment to clarify some things that are getting a lot of notice on social media and in the news media too. There’s a lot of talk, including from the Georgia Governor, that schools can reopen safely based on some recent studies by CDC and statements by the CDC Director, Dr. Rochelle Walenksy, where she stated that “vaccinations are not a prerequisite” for safe school reopening. However, what’s being lost is the second half of the message from CDC’s studies and Dr. Walensky’s comments - we have to have the right mitigation measures in place and a strong commitment to safety culture both inside and outside of the building. Those conditions don’t exist for a lot of Georgia counties due to lack of community commitment and lack of resources for schools.
In addition, there’s a growing debate over whether K-12 teachers and daycare staff should be prioritized for vaccination in order to get schools reopened for in-person learning. And I’m seeing more chatter that teachers are trying to “cut in line.” As the Governor rightly points out, there is not enough vaccine to protect everyone we might want to protect right now. However, the way that teachers are being depicted in this debate is wrong. They aren’t trying to cut in line. CDC recommended that K-12 teachers and daycare staff were supposed to be in phase 1b alongside first responders, those 75+, and other frontline essential workers such as grocery workers, food and agriculture, transportation, etc. This was meant to take place ahead of those 65 - 74.
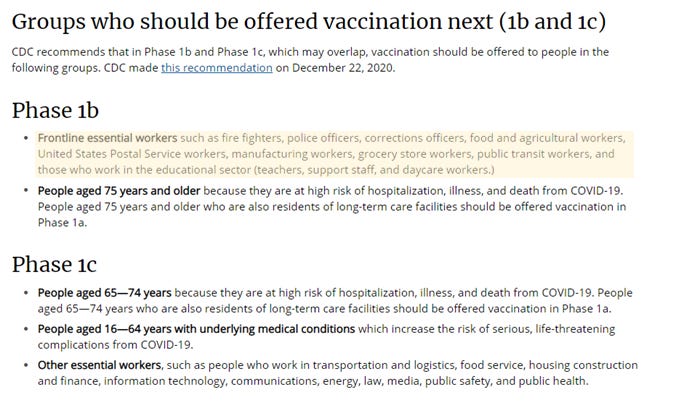
The Governor and DPH made a different choice, right or wrong, diverging from the CDC recommendations. They blended phases 1b and 1c and there were winners and losers in that determination. People 65 - 74 won and were moved to the front of the line alongside firefighters and police. All other essential workers (grocery, food and agriculture workers, public transit and educators) lost and were pushed to a later phase than recommended. Teachers and the other essential workers displaced by this decision are allowed to disagree with the Governor’s choice. It doesn’t mean that they are “cutting in line.” It means that someone else was allowed to cut in front of them.
And that might be okay if there wasn’t also this big push to reopen schools. After all, we *can* do school remotely while waiting for additional vaccines. As Dr. Walensky pointed out, vaccinations might not be a prerequisite for safe school reopening if other criteria are met. However, we aren’t meeting those criteria until we get community buy in to limit transmission and until we get the funding needed for schools to implement important safety measures against COVID-19. If the state and communities aren’t willing to commit to meeting those criteria, then they need to prioritize vaccinations for teachers.
Leaders are having to make really hard decisions and I don’t envy them. Let’s just make sure we’re being fair in the way we’re describing people in these debates and listening to the ENTIRE message from CDC.
References
https://www.legis.ga.gov/api/document/docs/default-source/senate-budget-office-document-library/appropriations/2021/afy21_sac_full_final.pdf?sfvrsn=27faebed_2
https://www.vice.com/en/article/qjpmp7/anti-vaxxers-misuse-federal-data-to-falsely-claim-covid-vaccines-are-dangerous
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-01/06-COVID-Shimabukuro.pdf
https://www.nbcnews.com/health/health-news/j-j-applies-emergency-authorization-fda-expected-greenlight-coming-weeks-n1256719
https://healthdata.gov/dataset/covid-19-reported-patient-impact-and-hospital-capacity-state
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations.html
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.