

The COVID Digest, 26May2021
Georgia COVID-19 Updates

Vaccine Update
The data provided in the table below are publicly available from the CDC update as of the morning of 26May2021. The table compares Georgia’s data to the US average. CDC indicates that Georgia has an inventory of 3,193,320 doses on hand. This week, the state has the 2nd largest stockpile of unused vaccines, 41% higher than the national average when adjusted for population. This week Georgia stayed the same or lost ground in the rankings across most metrics presented below. The one spot where Georgia gained ground was for vaccine completion among the 12+ population, moving from 47th place to 45th. Considering the 65+ populations, the state only saw first doses rise less than 1% this week. Meanwhile, only two thirds of this age group is fully vaccinated.

Yesterday Georgia Governor, Brian Kemp, issued a new executive order that prohibits state government agencies (including schools and universities) from requiring proof of COVID-19 vaccination prior to return to school in the fall. Before I read the article or executive order, I figured this was because the vaccine has not yet received full FDA approval (although this expected to be granted to Pfizer within the next month). That would have been understandable. Instead, I was surprised to see this statement as the logic for the decision:
I can understand that taking an authorized (but not approved) COVID-19 vaccine is something each person should weigh carefully and that their physician can be a trusted source of information in that decision making process. But the words chosen here have implications beyond COVID-19. They are a concession to the anti-vaccine movement more broadly. The state of Georgia already requires several vaccine series to be completed or underway before admission to K-12 schools, preschools and daycares. Similarly, there are vaccines required for incoming college students. However, if vaccination is now a choice for a citizen to make with their medical professional, then will the state no longer require vaccinations for children to enter schools? And is the Georgia Department of Public Health on board with this? Noticeably absent from the statement and the executive order is any statement or acknowledgment of the DPH or its commissioner, Dr. Kathleen Toomey. I think we can assume from their silence that they were not involved. The executive order also erroneously states that all Georgians above the age of 16 are eligible for vaccination. Every person over the age of 12 is now eligible. It’s another data point on analyzing how well thought out this executive order was.
The Atlanta Journal Constitution’s Greg Bluestein rightly called this out as a political move to improve his standing with his conservative base ahead of next year’s gubernatorial election. Governor Kemp frequently likes to accuse other people (including public health professionals) of playing “pandemic politics” in his statements and press conferences, including those who ask him why Georgia ranks so poorly on vaccinations. But holding leaders to account is not pandemic politics. Pandemic politics is making public health decisions based not on data or science but on whatever is politically expedient at the moment. And the Governor appears to be playing pandemic politics a lot over the past year. Public health is inherently political, as much as those of us in public health are trained to be apolitical. But the public’s health is not and should not be treated as a political football. The stakes are too high. The public’s health is not a means or ransom to securing or maintaining power. These are lives and families at stake.
I don’t know if this is just a political stunt with little foresight into the broad-ranging implications, poorly chosen words (despite a communications team and public health department to help him) or part of a larger effort among the well-funded and well-organized anti-vaccine movement to lead a Supreme Court challenge to up-end public health law as we know it. But it is not okay. Vaccines save millions of lives each year, including among the poor and disadvantaged - some of the same people who depend on public schools for educating their children. If you thought it was ethically challenging to decide whether to send your child to in-person learning this year during COVID-19, imagine the fear and anxiety that parents of children with medical conditions face when we fall far below the herd immunity threshold for things like measles and pertussis. These are diseases where we still see outbreaks. In fact, in 2019, the year that the pandemic began, we saw outbreaks of measles that resulted in the biggest annual US total since 1992.

Full disclosure, I did my post-doctoral fellowship in the pertussis and diphtheria laboratory at CDC while I was pregnant with my first child. I read autopsy reports for infants as part of investigating which molecular subtype of Bordetella pertussis killed them. As my baby kicked in my belly, I read the autopsy description of the infant’s hair color and sent prayers of comfort and solace to their parents. So pertussis matters A LOT to me. When my child was born, anyone who wanted to hold him needed to show me proof of Tdap vaccination. Vaccine passports are not new. We created as tight of a cocoon around our son as we could until he could receive his vaccines, because someone else’s momentary happiness over holding our baby was not worth his life. And I view COVID-19 vaccination in much the same way as people have begun to try to push their risk tolerance onto my family. I digress, but I thought this background was relevant. The graph below from CDC on pertussis incidence is powerful for two opposite reasons. First, look at how badly pertussis used to impact the American population each year before the advent of the vaccine (see arrow labeled DTP). Look at how dramatically the cases dropped over the following decades, from a high of 265,269 in 1934 to a low of 1,010 cases in 1976. It took decades, but pertussis was reduced by 99.6%. Contrast that to more modern history when we peaked at 48,277 cases in 2012 and saw 18,617 cases in 2019. Vaccines are powerful life-saving tools. But they are not perfect. If we have problems with waning immunity (this is the case for pertussis) or if not enough people are vaccinated, outbreaks can and will happen.

As is often the case, the people who could be hit hardest by this slippery slope of shifting vaccine policy will be those who have been medically underserved all along (including people of color and rural communities) as well as families with someone who is immunocompromised. The privileged, who have stable access to care, will be able to access that care if a local outbreak of vaccine-preventable disease impacts them. That won’t be the case for many of Georgia’s children. Statements like the Governor’s are part of a continuing theme over decades: that public health does not matter to the people in power in Georgia. The state’s population (especially the poor and medically underserved) pays the price.
The United States

The map above comes from the CDC COVID-19 Tracker on the Community tab, county view. The map above looks at the combined community transmission indicators that looks at both case rate and test positivity. Red and orange are considered the danger zone, yellow is safer and blue is safest. Things have improved a lot in many parts of the country, including in Georgia.
The table below tells you where we are this week and how that compares to the previous week (in parentheses). The data for everything comes from the HHS Community Profile Report from 25May2021.

Georgia has two counties in the top 20 counties in the US for new case rate per 100,000 residents. They are Chattahoochee county at #2 and Charlton county at #9. Chattahoochee is likely an overrepresentation of cases (and vaccinations when we review those data) among military personnel temporarily residing on Fort Benning for training compared to the census of the population (where the temporary trainees are not counted).
The table below shows the highest and lowest ranking states and territories from the latest HHS Community Profile Report (you can find the most recent edition here).

Georgia appears twice in this table, with the 5th worst hospital admission rate in the country and the 4th worst death rate. Nationally, there is only one state in the red zone for any metric (Delaware for case rate). I also want us to look at the worst states for vaccinations. Notice that for residents 65+, the worst “states” are actually US territories. These areas may have significant challenges with obtaining and storing vaccine and clearly are having difficulty reaching their senior population. However, if we look at the worst states for all residents receiving at least one dose, the only US territory there is the US Virgin Islands. In fact, Guam is already >50% of its population with 1+ dose. Southern US states (MS, LA, AL) and Wyoming are doing a worse job of vaccinating their population than US territories that are not part of the continental United States.
Georgia
We can zoom in on a current view of Georgia using the CDC community transmission criteria. This week, there are 12 red counties and 31 counties in the orange category. So there are 27% of the state’s counties in the substantial or high transmission categories (last week it was 50%). Nationally, 45% of US counties are in the red or orange zone. So Georgia is performing below the national average, in a good way.
This week, the entire Atlanta metro has shifted to yellow. There’s a lot of improvement, actually, in this map.

Testing
If we drill down to Georgia in the HHS data, we can see the following test positivity rate by age group in the chart below. There’s improvement for all age groups compared to last week. And only 12-17 year olds are above the 5% goal line. We need to not brush off symptoms in this age group and seek testing. In the meantime, we are undercounting disease among these adolescents.
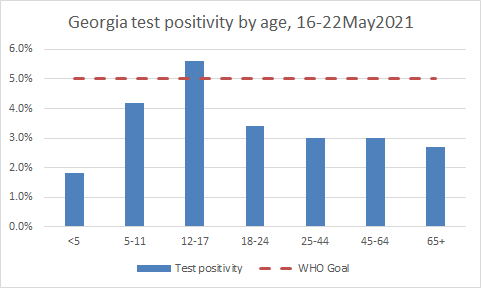
It was a typical (and low) testing output day for Georgia. Test positivity was 2.7% for PCR tests and 2.1% for antigen tests.
Cases
Today there was a net increase of 549 newly reported cases for Georgia, with 388 identified by PCR and 161 by antigen testing. The state’s case rate is decreasing, and sits at a level we haven’t seen since 01Apr of last year.
Hospitalizations
Today there were 141 newly reported COVID-19 hospital admissions and 32 admissions to the ICU. The COVID-19 data hub for patient census is not working for the past two days. I’ve notified my colleagues at the state’s COVID-19 Data Task Force and hopefully we’ll have data on this soon. In the meantime, HHS also tracks this for the state. Here’s how the graph looks using those data.

Deaths
Today Georgia reported a net increase of 24 newly reported confirmed COVID-19 deaths and 12 probable deaths. The state’s death rate per 100,000 is now 28% below the pre-winter surge baseline, (last week 54% below). So death rate is higher this week than last week. Let’s work on getting vaccinated so that we can prevent as many of these deaths as we can.
References
https://covid.cdc.gov/covid-data-tracker/#vaccinations
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
https://www.ajc.com/politics/politics-blog/georgia-governor-bans-state-government-from-requiring-vaccine-passports/EHCLAVN6JFAGZLEJTK3CXZSMF4/
https://dph.georgia.gov/document/document/immunization-requirements-georgia-child-care-and-school-attendance/download
https://beta.healthdata.gov/dataset/COVID-19-Reported-Patient-Impact-and-Hospital-Capa/6xf2-c3ie
https://www.nature.com/articles/s41591-021-01260-6
https://www.unicef.org/media/media_102809.html
https://www.cdc.gov/pertussis/surv-reporting.html
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.