

The COVID Digest, 17Sep2021
When public health becomes personal

As this delta surge begins to wane, the big data item to track right now is COVID-19 deaths. The graph below shows how cases (left y-axis), hospitalizations, ICU admissions and deaths from COVID-19 (all on right y-axis) have compared over time.

In Georgia, here’s how the metrics changed in the past week compared to the previous week:
Cases decreased 19%
Hospital admissions decreased by 3%
ICU admissions rose 8%
Deaths rose 21%
ICU admissions and deaths have always trended behind cases and hospitalizations. This has to do with how long it takes for an infected person (a case) to become seriously ill and pass away from COVID-19. It can also be impacted by delays in death reporting, which is common in public health. As an example, this week Georgia DPH reported a COVID-19 death in a 5 year old boy from Gordon county. The details are similar to a story previously reported in July by the Atlanta Journal-Constitution. If the newly reported death is for the same little boy, then you can see that it took about 2 months for us to see it in the data. My deepest condolences go out to his family, community, and the medical team who likely tried everything they could to save him. I’m so sorry for your terrible loss.
Something interesting is going on with testing. Despite a huge drop in PCR testing volume (51% less than the previous week), the test positivity rate continues to decrease. A less stark decline in antigen testing volume also resulted in a drop in test positivity rate.
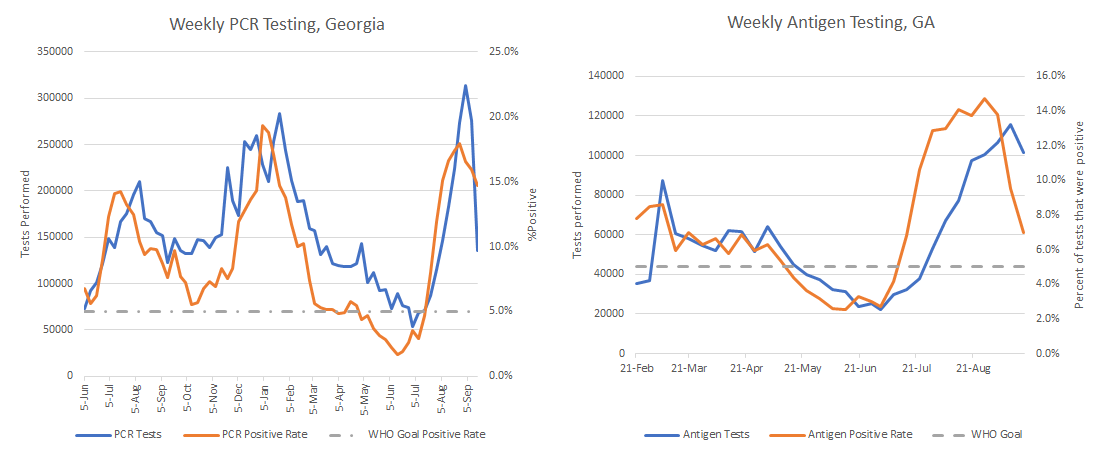
This would make it seem that the case drop that we’re seeing is real. If you remember, evaluating the data as the tide turned on this surge was difficult because of the Labor Day holiday. We didn’t know if perhaps a decrease in testing was the explanation. We are seeing a decrease in test volume. But the positivity rate is also decreasing. So this might suggest that even though testing volume is down, there are fewer cases out there to “miss” with current testing capacity if the case drop is real.
The graph below shows the 7-day case rate per 100,000 residents for each of the 14 hospital regions in Georgia and the statewide average. You can really see the impact of the Labor Day holiday with the weird spike in the past week or so. Tests get held for the holiday, meaning fewer tests/cases reported. Then labs work through the backlog and report a bigger test/case total than usual.

Despite that blip in the data, we can see that case rate has remained steady but low for hospital region D (Atlanta) and now other regions are descending to the region D rate.
Cases are decreasing for every age group except infants under the age of 1, where the case total is about the same as the previous week, 279 PCR cases in the past week. Another sign of good news on this graph is that the unknown category shows a negative number.

The unknown category is a holding spot for cases that are pending investigation and follow up by contact tracers and public health departments. So seeing the number go negative means that not only is the current case load something they can manage, they’re making headway against the backlog too.
Cases are declining among K-12 aged children which is a really good thing. You can review the data from the Georgia Department of Public Health in their School-Aged Surveillance Data Report.
Burden on hospitals remains high, but it is getting better, albeit slowly. The graphic below shows how each hospital region is doing for ICU bed usage and COVID-19 patient census (or how much of their patient population is hospitalized due to COVID-19).

Hospital region D (Atlanta) is the first to drop out of the dark red zone for patient census. For three weeks, every region in the state was in the dark red zone. At the delta wave peak, preventable COVID-19 infections accounted for 35.7% of the state’s hospitalized patients on 07Sep2021. There are four regions using an excess of ICU beds - regions C, F, I, and M. In fact, region M has been in this situation everyday since 12Aug2021. It’s a lot of strain for a sustained period of time.
Hospitalizations are not dropping as quickly as cases though. In fact, for some age groups we continue to see rising hospitalizations: 10-39 years old, and 60-69. Mercifully, the increases are a lot smaller this week for these age groups than we’ve seen in recent weeks.

Considering how overburdened hospital region M has been for ICU bed usage, it is perhaps no surprise that the region has experienced the worst COVID-19 death rate in the delta wave, by a large margin. Region M’s 7-day death rate is 31% higher than the next highest region (K, southwest Georgia) and 540% higher than region N (northwest Atlanta suburbs), which has the lowest death rate in the state.

As mentioned at the beginning, confirmed deaths rose by 21% this week. It’s possible we may see a new record next week although I certainly hope we do not. If we look at this week’s deaths by age group, we can see that deaths rose for all adult age groups. Some of the largest relative increases were seen in 18-29 year olds (+250%) and 50-59 year olds (+40%).

On Monday I received the phone call from the school telling me that my 10-year old was the close contact of a confirmed COVID-19 case at school. His entire class was placed into quarantine for 14 days from the last known exposure. Using the store-bought rapid antigen tests, he remains negative for COVID-19 7 days post-exposure. Hopefully he remains that way. But it has meant a lot of chaos for this dual working parent family as we try to juggle teaching schedules. I know many of you have already dealt with this situation. It just happened to be my turn.
The other complicating factor is that the Kansas legislature, passed a law that public schools could no longer offer a virtual learning option on a permanent or even temporary basis to students (i.e. virtual learning during quarantine). So my son’s class is not receiving instruction for 14 days other than what the teacher can push to Google classroom, but there is no audio or video content allowed from the teacher. No Zoom, despite a really successful year of online learning last year.
And perhaps this wouldn’t be a big deal if it were a one time problem. But until he becomes eligible for the COVID-19 vaccine, he could return to school after quarantine and get sent back home almost immediately for another 14 days if another child brings COVID-19 into the classroom. So losing a month or more of education just seems like we’re back to square one, March 2020, trying to make it work without proven tools for virtual learning. What upsets me most is that the reason we are here is not because our school district lacks the tools and resources for virtual learning (every child has a Chromebook). In fact, the school is as frustrated as we are. The reason my child can’t learn with the best that my school district has to offer is because of the anti-science COVID-denying faction that dominates the state politics where I live. It’s just one of many examples where it seems like we’ve learned nothing from the gains we made during the pandemic. There was a lot that was awful about the pandemic. But there were good things that we might consider keeping. Being anti-progress holds all of us back, especially as this pandemic is very much NOT over.
I talked about this experience a bit this week on Georgia Public Broadcasting’s Political Rewind show. Thankfully, my son slept through the whole experience and the dog was quiet too. Hopefully we can continue to be lucky and avoid COVID-19 for my son until the vaccine is approved for children.
The COVID Digest is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available. Many thanks for your support!
My Ph.D. is in Medical Microbiology and Immunology and I am Chair of the Division of Natural Sciences and Mathematics at the University of Saint Mary. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion, do not represent the views or opinions of my employer and should not be considered medical advice.