

The COVID Digest, 17Jul2021
Georgia COVID-19 Updates

Hello readers! I regret that my new position has limited my time for writing. It is my hope that as I settle in, I will be sending more frequent newsletters. The University is very supportive of the work I’m doing and is hosting a webinar for me to speak to the campus and the public about the importance of vaccinations for college communities. You can register for the event here. In between my newsletters, I do provide updates and commentary on Twitter. You’re welcome to follow me there too.

This week, all four of the big metrics increased for Georgia
Cases +70%
Deaths +38%
Confirmed hospital admissions +34%
ICU admissions +28%
I believe this is the beginning of the delta variant’s impacts in the state. Tomorrow marks 2 weeks since 4th of July. So this coming week is when we should begin to see cases and hospitalizations that resulted from that big social event. I would not be surprised if we see really big numbers starting this week.
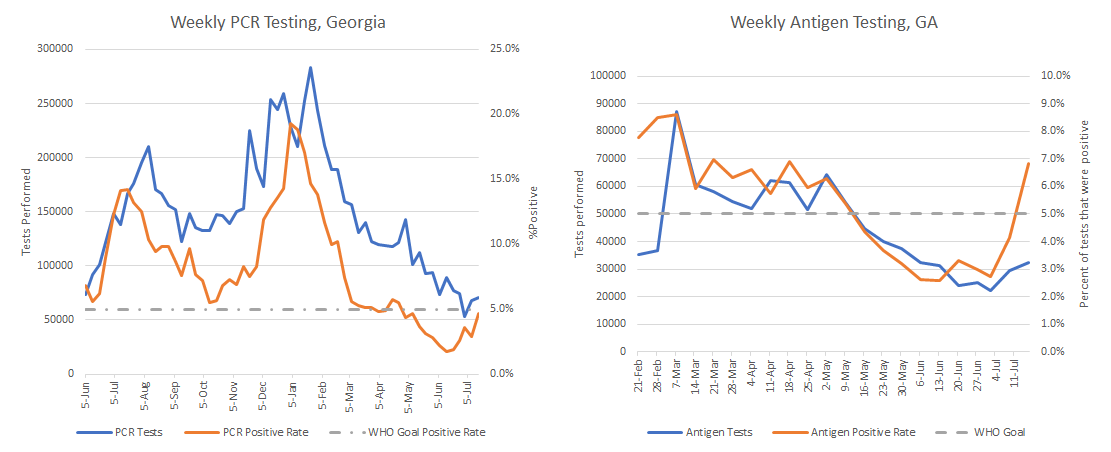
Let’s look at testing
In both graphs below, the blue line represents the total tests performed (weekly) and the red line shows the percent of those tests that were positive. Antigen test positivity skyrocketed this week, well above 5%. PCR test positivity rose to just under 5%, despite the fact that testing overall increased. I’m glad that testing output increased, but it will need to increase more to keep up with disease transmission rates in the coming weeks.
Statewide, the patient census for COVID-19 is rising
It is rising most dramatically in hospital regions D (Atlanta), H (Dublin - Milledgeville), J (Savannah and coastal Georgia), and M (Waycross and surrounding areas. In other words, things are most intense in the southeast region of the state. But even Atlanta, with its higher vaccination rates, is seeing significant increase.

Will counties with higher vaccination rates be protected?
The problem is that even the highest rate county in the state (Oconee, just over 50%) is a long way off from the 85-90% we need. Yes, there have been a lot of infections too, and that’s a route to immunity, but I do not think we have sufficient population immunity to prevent a surge even in higher vaccination rate communities. And I certainly wouldn’t assume that you don’t need to take precautions if you’re in a county with not-awesome-but-better-than-zero vaccination rates. In fact, if we look at Missouri where two of the counties have similar vaccination rates to Oconee (see the blue stars), we can see that even they are now in the red or orange zone for community transmission levels.

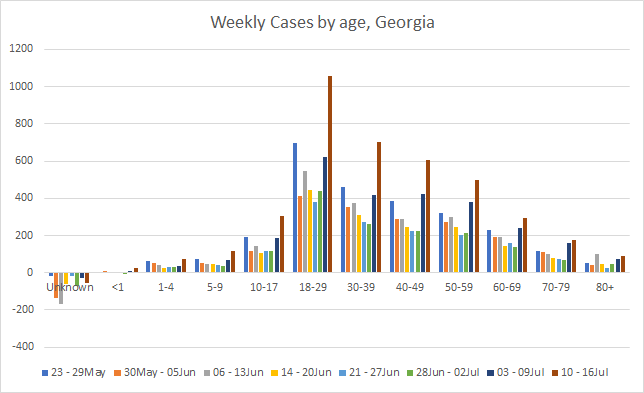
Where are cases coming from?
Back to Georgia, case rate is rising most for rural counties, many of which have lower vaccination rates and greater difficulty accessing a hospital. So it’s reasonable to predict that these counties will be hit hardest with hospital demand and death, but I would not assume that any counties are “safe.”
Let’s take a look at where these cases are coming from in terms of age group. Cases jumped the most this week in the 18-29 year old group. Historically, every surge has begun this way, beginning with young adults and then fanning out to all other age groups. If we want to save the most lives, we vaccinate those 65+ (which the US and Georgia have prioritized). If we want to end the pandemic, we need to vaccinate young adults. Because surges start with them. Please note that while cases are rising most among 18-29 year olds, they are rising for those 60+ too. So despite the incredible progress that the US and Georgia have made in vaccinated those populations, it has not been enough. The 60+ age group has a cumulative hospitalization rate of 21% and a fatality rate of 9.1%.
But what’s happening in Missouri and elsewhere is that the people in the ICU this time around are younger - 20 to 40 year olds. Below there’s a clip from Ed Yong’s recent piece in The Atlantic. Please don’t mistake youth with invincibility.

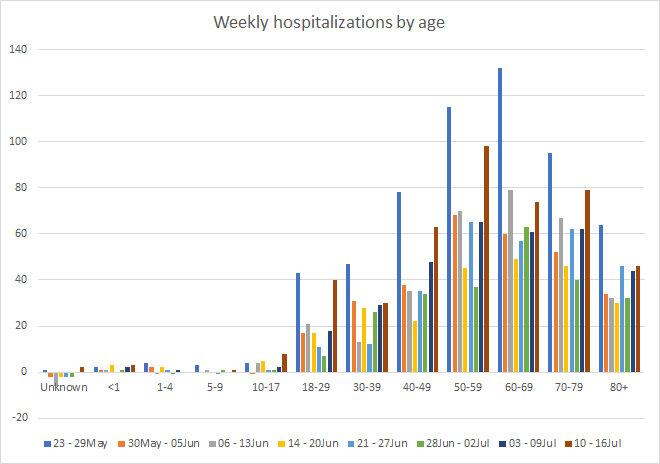
Hospital admissions are rising most for those 18-29 and 50-59.
An update on breakthrough infections
Last week, the CDC updated their numbers on breakthrough infections associated with hospitalization and death now that 157 million people have been fully vaccinated in the US. These are infections that occur despite a person being fully vaccinated. Some cases are to be expected. The Pfizer and Moderna vaccines had an efficacy of >90% in clinical trials. That doesn’t mean that 10% of those vaccinated will contract the virus. What it means is that a fully vaccinated person’s risk of infection is 90% less than someone who was not vaccinated. That will also vary based on how well a person’s immune system functions. It’s important to remember that what CDC counts as a breakthrough infection is likely a significant undercount because they don’t recommend testing fully vaccinated people following exposure. This is just what we happen to know. Some of the hospitalizations and deaths noted were positive at the time, but their hospital admission or death was unrelated to COVID-19. For example, they were screened for COVID-19 on admission for a car accident, etc. However, we’re including those individuals anyway so that we can see the worst case scenario.
So let’s say we want to get 157 million people to immunity. You can choose to get to immunity through vaccination or natural infection. Let’s compare the risk with both strategies, using the cumulative hospitalization and death rates we’ve noted for Georgia for natural infection.

157 million cases would mean 9.1 million hospitalizations and 3.2 million deaths. By comparison, 157 million fully vaccinated persons have had 4,909 hospitalizations and 988 deaths to date. Vaccination is far and away the safer path to immunity. In the meantime, we have a lot of people who can’t access that path including those who are immunocompromised and children under the age of 12. We protect our kids and those who are immunocompromised by creating a protective cocoon of vaccinated adults (or those aged 12+) around them.
I had hoped that we would see an EUA for kids under the age of 12 by September, but news came out this week that EUA for vaccines in this age group are expected to come in midwinter. This is pretty profoundly disappointing for parents who are preparing to send their kids to in-person learning, many of them in school districts that never treated the pandemic like the threat that it was and have abandoned all remaining protective measures that were put in place. Parents are in an impossible position. Despite how much government at all levels has pushed and prioritized in-person learning (and for good educational and social reasons!), they have not prioritized the investment in safety infrastructure that is necessary to make that in-person learning successful and safe. If you want to protect these kids and keep them in school, get vaccinated and wear your mask, even if you never enter a school building. Because disease doesn’t stop at the school’s front door. Community transmission impacts school transmission.
So if you’re part way through your vaccine series, be sure to get that second dose on the very first day you’re eligible to receive it. If you’re not vaccinated, please initiate that process today and wear your mask and avoid indoor crowds until you’re 2 weeks post-second dose. It’s not for forever, but I want you to be safe.
Of note, 75% of the breakthrough infections were noted among people aged 65+. This makes sense and agrees with the clinical trial data. If we consult the table below that compares those adults under 65 and those above 65, we can see that vaccine efficacy is still really high, but reduced for those 65+. This is thought to be a function of normal human aging - the immune system starts to decline at about age 65.

Just remember that the vaccines are very powerful tools, but they’re not perfect. Even if you’re fully vaccinated, you need to add layers of protection during case surges such as the one we are experiencing with delta. When the case surge recedes, we can begin to slowly remove layers of protection and rely more heavily on the vaccines. But there just aren’t enough people vaccinated at this point to rely upon them alone to protect community health.
So what do we do?
We’ve had the benefit of time and the ability to prepare for delta as we watched what was happening in Missouri. But I worry that our time is running out. Earlier this week, I spoke to the Georgia Municipal Association, a collection of mayors, county commissioners, city councilmembers, and other public servants. The advice I gave to them was somber - prepare for this with the seriousness and intensity that you reserve for a major hurricane. Surge vaccinations and test capacity, work with your health department to recruit contact tracers, make sure your EMS and 911 services are fully staffed and supplied, encourage vulnerable citizens to avoid indoor crowds regardless of vaccine status, encourage multi-layer disease protections (including masks). Because the mass casualty event happening in southwest Missouri is not what we want for any part of Georgia.

How bad will this surge be? On the one hand, I’d like to think that because we prioritized vaccinating those 65+, we might not see as many hospitalizations and deaths as last time. But SW Missouri has seen their COVID-19 patient census rise to the same level as their peak during the winter, when vaccines weren’t widely available. In the UK, their case count is approaching the peak that they experienced in winter as well. Delta is a game changer for the virus, readers. A lot of this will come down to how fast we can halt exponential growth of cases and hospitalizations. In the past, it seemed like when news coverage really honed in on how serious a surge was, we peaked soon after. I suspect that people heard stories of overwhelmed hospitals and limited their exposures. But the news coverage has been focused in Missouri and things continue to intensify locally.
But while Missouri is currently the main area of focus for the delta variant in the US, I worry that ultimately this news story will be focused on the South. Because I fear that the South is going to be hit even harder. Missouri is considered part of the Midwest by the US Census Bureau (purple line in the graphs below), but the South has the highest test positivity and hospital admission rate by a large margin.

What about the kids?
The other question I’m being asked is what am I doing for my own, unvaccinated child. We have prioritized our best masks for him to use and he wears a KN-95 any time he is indoors with non-household contacts, which we limit as much as possible. The rest of us, who are fully vaccinated, are wearing cloth masks during our indoor encounters with non-household contacts particularly when we don’t know someone’s vaccination status. We do not do any indoor dining and are limiting our errands. Our school district removed all virtual learning options for the fall but were very good about masks last year. I’m hoping that will continue this year. Trust me, the whole family is eagerly awaiting mid-winter when we might expect a vaccine for those <12. We had planned a vacation in September that would require an airplane, thinking that surely there would be a vaccine for kids <12 by then. But with the postponement in EUA for children and delta surging in many parts of the country and the world, I am considering delaying that trip until next year.
Like I said earlier, parents are in an impossible position. Governments (at all levels) have decided that our children are the risk they’re willing to take for economic recovery.
Meanwhile, the Tennessee Department of Health has stopped outreach for all pediatric vaccines (not just COVID-19) due to political pressure and the anti-vaccine movement which is capitalizing on the politicization of this pandemic. If we think disease control is difficult and expensive for COVID-19, it pales in comparison to what it takes to control an outbreak of measles. I would be very wary of politicians, YouTubers, TV personalities, and so-called experts, etc, who are pro-disease after all that we have been through. How do we possibly benefit from mass death? Dead people don’t vote, don’t contribute to TV ratings, clicks/shares on social media, don’t pay taxes or contribute to the economy, etc. If you wouldn’t ask these pro-disease people about your diabetes or allergy medication, you should not be seeking their advice about a vaccine. Please talk to your medical provider regarding medical decisions.
Make good choices, be safe and be well. Remember that our protection right now is multi-layered.

The COVID Digest is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology and I am Chair of the Division of Natural Sciences and Mathematics at the University of Saint Mary. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion, do not represent the views or opinions of my employer and should not be considered medical advice.