

The COVID Digest 12Feb2022
The futility of COVID denial

Good afternoon! This week’s COVID-19 digest will include a round up of national and regional trends followed by a commentary on the state of the pandemic.
We’ll use this snapshot of the national metrics from the New York Times Coronavirus Tracker to get started today. Using the red graph, we can see that cases are continuing to fall nationally by 77% since the peak set on January 14th. Meanwhile, the average daily cases are still higher than the peak of the Delta wave in summer and fall of 2021.
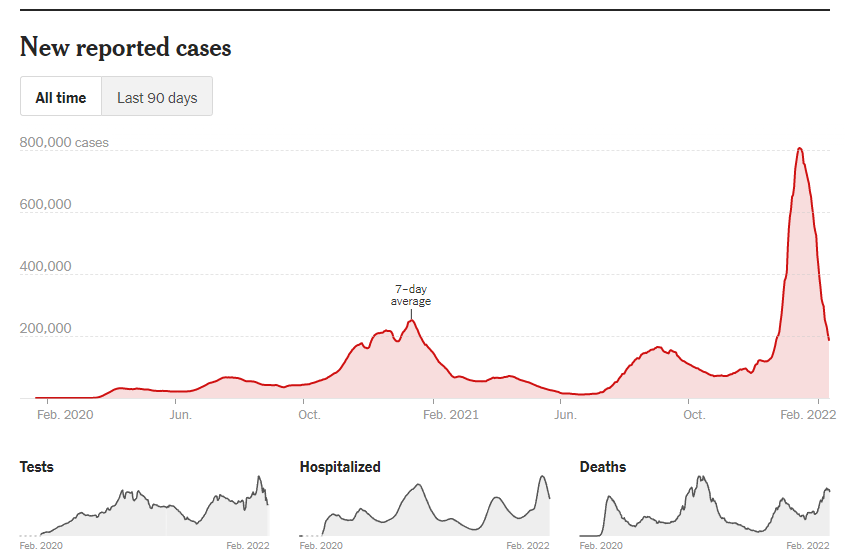
Testing is also declining. This could be because fewer people are experiencing symptoms or also because people are shifting to home tests that aren’t typically reported. Hospitalizations have declined to about the level of the Delta peak. So while things are certainly better than they were a month ago, they remain quite intense. Lastly, deaths may have begun to peak. However, its very possible that delayed reporting may drive this curve upward. In addition, I’m hearing a lot of talk among physicians that while Omicron may have been milder in its initial infection, it leads to complications that are pretty serious after the infection itself is gone, like strokes, blood clots, etc. However, if this is the peak of the Omicron deaths, this wave remains the second deadliest of American history with the COVID-19 pandemic, even with vaccines widely available. Sixty four percent of the US population is fully vaccinated according to the New York Times tracker.
If we look more regionally using the Department of Health and Human Services Community Profile report from 10Feb2022, we can see that indeed hospital admissions are declining everywhere.
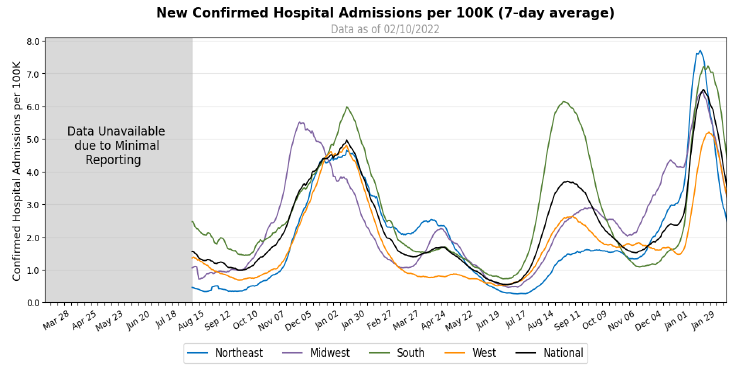
But there are somethings I want to highlight here. First, the rate of descent for the Northeast is slowing at a rate higher than they entered the Omicron wave. We can also see that not all regions have been hit equally hard. The data only goes back to August 2020, when hospital data became complete enough to track. As you may recall, the Northeast (particularly New York) was hit very hard in the spring of 2020. But they were not the worst off in the winter of 2020-2021, nor during the Delta wave. They were the top region for the Omicron wave, however. The Northeast and the West had similar experiences for the winter 2020-2021 wave, but the West had a more dramatic Delta wave. Finally, for Omicron, the West peaked at a hospital admission rate that was about 30% less than for the Northeast. The Midwest initiated the winter 2020-2021 wave, passing the baton to other regions, where the South was ultimately the top region. The Midwest was middle of the pack for the Delta wave, which is interesting since it seemed to really get going in Southwest Missouri. Ultimately, the Midwest was middle of the pack for the Omicron surge. The South was the hardest hit for the winter 2020-2021 wave, again for Delta and nearly the top region for the Omicron surge.
Why are the regions having such different experiences during these waves? It is likely a combination of factors, but two things stand out to me. First, clearly, things don’t have to be as bad as they have been. There are regions that were able to escape the worst of things either through better disease containment, vaccination rates, or public health policy. Second, for those who are advocating for the herd immunity approach, it’s pretty clear from the South’s example that it’s not going to happen. The let everyone get infected model has led to successively worse burdens on hospitals with each wave. The virus is evolving around natural and vaccine-mediated immunity. Let’s do better.
There’s been a lot of talk lately about the need to get back to “normal,” which I can only assume means life in 2019 prior to COVID-19’s arrival in our lives. First, there’s the erroneous assertion that COVID-19 is mild, like a cold. Cold-like illness doesn’t cause the hospital spikes we’re seeing in these waves. Cold-like illness doesn’t kill 900,000 Americans. Next, there’s the assertion that people have had the chance to get vaccinated and “I’m no longer going to be inconvenienced” for those who have chosen not to do so. First, I would remind you that even if you’re fully vaccinated and boosted, you are much less likely to need a hospital, but there is still a non-zero chance that you’re going to catch COVID-19 and mild just means you’re not going to a hospital. Second, there are people who are doing all the “right” things in your eyes but are unable to mount a full immune response. Third, there are still a lot of people (ages 5 and under) who aren’t even eligible to be vaccinated in the first place. In addition, there are a whole host of children who aren’t vaccinated through no fault of their own. They are too young to legally consent to a vaccine. It is their parents making that decision for them. Please say with a straight face that children risking disability and death in rare cases is the price you’re willing to pay to no longer be inconvenienced. If you think of yourself as a “good” person, I want you to imagine saying these things to a person who lost a loved one to COVID-19. Tell them that their pain and anguish is “mild” or “not a big deal” compared to your privilege to ignore this problem. I’ll date myself here, but when I was an adolescent, those “What Would Jesus Do” bracelets were everywhere. And I often find myself looking around at all of these Christians who are my same age and think, “really? This ambivalence is what you think Jesus would do? Do you honestly think He would see this suffering and death, shrug and say ‘well, it sucks to be you?’”
Remember this newsbyte from 2020 that was among the first to suggest that certain populations were disposable or worth sacrificing for the US economy?

In two years this idea went from whacky to mainstream as people got tired of caring about other people and politicians were ready to talk about something else rather than face accountability for their own shortcomings in leadership. The difference now is rather than a handful of people saying they’d be willing to die for the almighty American dollar, a handful of people have decided *you* should be willing to die for the economy and for political expediency.
In addition to the moral depravity of this effort, it is also mired in futility. Imagine saying we’re done with hurricanes. We’re done with droughts. We’re done with forest fires. We are done with cancer. We’re done with paying the rent or the mortgage. These problems don’t cease to be problems because we’re tired of thinking about them. As you can imagine, it just makes us less prepared for those problems, allows those problems to become bigger problems that are even harder to manage. It is utterly preposterous for humans to tell a virus (that is evolving and not participating in conversation) that the virus is no longer a thing. We have the technology to make serious inroads against the virus for future surges. But rather than work to improve indoor air quality to limit the spread of illness, we’re going to continue to behave as though the virus is not there. We used to be a country of innovation and progress, and yet here we are hampered by ambivalence and defeatism. We will most likely need vaccine updates, kind of like how the influenza vaccine is updated each year, to maintain immunity against evolving variants because humans are continuing to allow that evolution to occur with low global and domestic vaccination rates. But US vaccination has stalled, so we need to anticipate that even if we update the vaccines we aren’t likely to see enough people get them to prevent future surges from happening.
Trust me, I am relieved to see cases and hospitalizations declining. There will be more things we can do during the lull between surges than we can when cases are skyrocketing. And trust me that I would also like to stop talking about COVID-19. But this pandemic isn’t over and probably won’t be for some time because humans cannot seem to get it together enough to confront the problem. Instead of having any level of certainty or control of this crisis, we are allowing the virus to control us through our collective inaction. We can ignore the virus and continue to have so many teachers out sick that the National Guard has to come in and babysit classrooms full of children. All the while, we’re ignoring that we are demanding that those teachers take on extraordinary risk for our benefit. If they refuse, people call them lazy and selfish. I would really like for people to care more about others and for that to be the intrinsic motivation for preventing disease. But you definitely don’t have the right to determine what risks are acceptable for other people. There is a talking point that we can’t let the unvaccinated hold the rest of us back. But abandoning all efforts to limit disease spread isn’t really sticking it to the unvaccinated (an absurd goal anyway). It is surrendering to the apathy and selfishness that motivates many of those who have denied the significance of COVID-19 from the beginning. 900,000 Americans have died and there are a lot of people who DO NOT CARE. What atrocities would they turn a blind eye to out of indifference? When we are as morally bankrupt and driven by conspiracy theory as we are as a society right now, I’m afraid to hear the answer to that question.
These surges are going to keep coming, probably on a twice a year cycle when climate is uncomfortable enough that people gather inside (summer and winter). When you don’t try to limit disease (use the South as an example) the surges will happen regularly and they will be severe. Every time they happen hospitals will be overwhelmed and people with cancer and heart disease and other conditions will have to defer care. More healthcare workers will leave the field, devastated by PTSD and burnout. Nursing shortages will get worse. That leaves us less prepared for subsequent surges also.
The pandemic exposed major weaknesses in our healthcare system and public health infrastructure. We can go back to the “good old days” of racial and socioeconomic disparities of health that fell under the radar of politicians, dismissed as “other people’s problems.” The pandemic brought those disparities right in front of our faces and it’s uncomfortable. Or we can learn from this pandemic and address these issues, resulting in a better healthcare system and public health network for everyone. Let’s recognize that there is no going back to 2019. Let’s look forward instead of backward. Let’s care about others.
Keep reading with a 7-day free trial
Subscribe to The COVID Digest to keep reading this post and get 7 days of free access to the full post archives.