

The COVID Digest, 07Aug2021
Georgia Update

It was another big week for the delta variant in Georgia. Let’s go through the numbers.

This week all of the metrics in the graph above increased. Cases are up by 47%, hospitalizations rose 28%, ICU admissions rose 17% and deaths rose by 146%. We often see a delay between the rise in cases/hospitalizations and the rise in deaths. In summer 2020, the delay was 3 weeks. In the winter surge it was 5. This time, it looks more like the delay we saw last summer. Keep in mind that death reporting is often delayed and this is a problem every week.
For testing, the number of tests performed for both PCR and antigen testing have risen dramatically (by 27%) for each compared to the previous week. Test positivity leveled off for antigen testing but continues to climb for PCR testing.

There were 31,990 newly reported cases this week between PCR and antigen-identified cases. During the week ending 09Jul (more or less a month ago) the weekly total was 3870. The case rate is most intense in rural counties in Georgia. Nonrural counties match the state average and Atlanta metro counties have the lowest case rate so far. But all are rising.

I’m not showing the data this week, but cases continue to climb across all age groups.
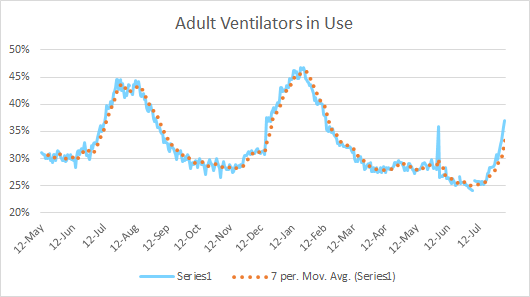
As we know from past experience, cases drive hospitalizations and deaths. After all, you can’t die from COVID-19 or end up in the ICU if you never got it in the first place. 857 people were admitted to Georgia hospitals this week for COVID-19. The state hasn’t seen a number that high since descending from the winter surge. The graph below shows us that ventilator use is also increasing fast. So not only are more people going to the hospital, enough of them are sick enough to require advanced care to move this needle. The state does not provide data on pediatric ventilator use.
The big increase in hospitalizations is distributed across age groups. This curve more or less matches the distribution for hospitalizations cumulatively, with a lopsided bell curve centered around 60-69 year olds.

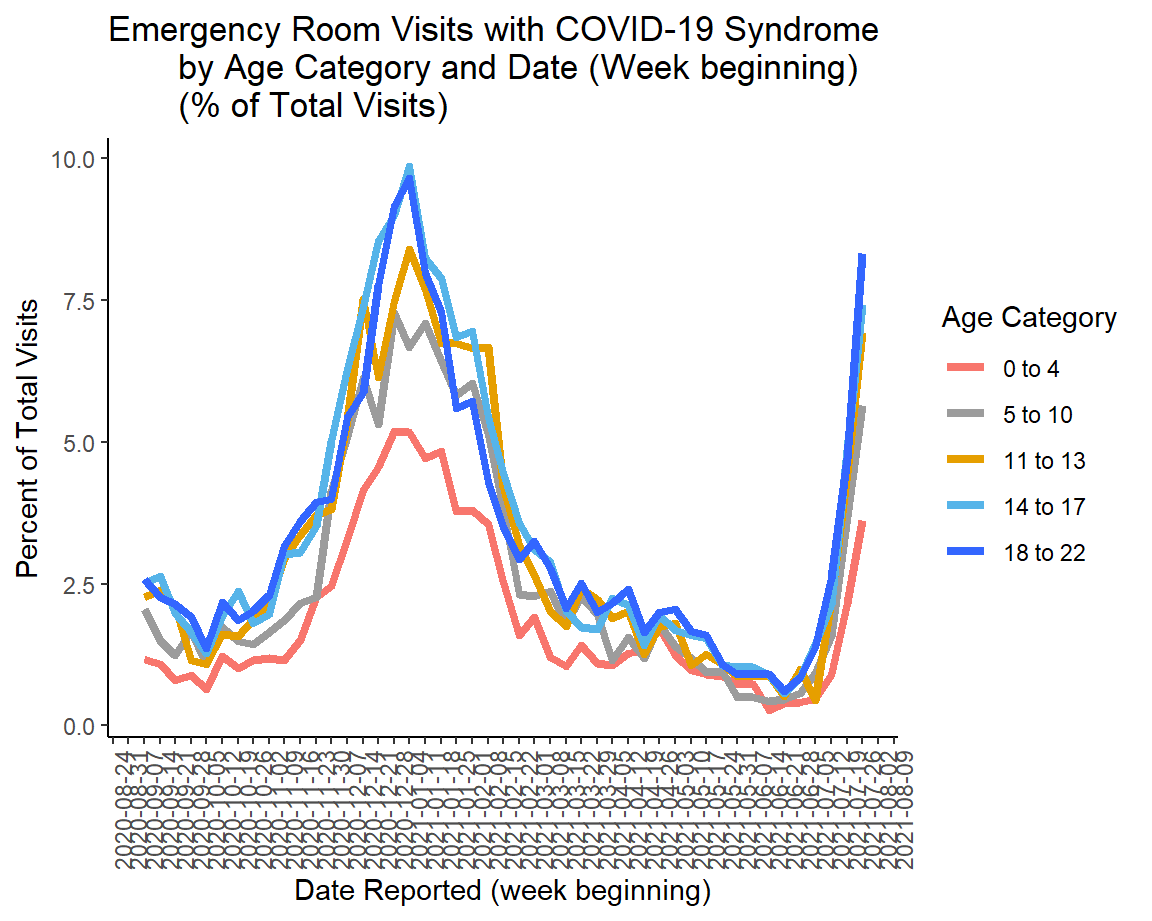
The graph above shows admissions - people sick enough to warrant an overnight stay in the hospital. We can look deeper at the pediatric population for those who needed an ER visit for COVID-19. Some of these may have been admitted eventually, but not all. What we can see is that all age groups are rising and approaching the previous maximum. Keep in mind, this represents data through 26Jul. So, before school began for most Georgia counties. We’ll have to wait to see what impact school reopening has on this graph and the one above.
There is a potential spot of good news. Some of the hospital regions are seeing patient census begin to level off. The graph below is for hospital region N (northwest Atlanta suburbs). Similar trends are observed for all regions other than regions D (Atlanta), G (Augusta and surrounding counties), L-M (southeast Georgia, Tifton, Valdosta, Waycross). It could be that there are fewer patients being admitted because there are fewer people sick. But it could also be that hospitals are being more careful about who they admit versus send home to manage in an effort to preserve bed capacity.

It’s too soon to know if this is a peak or a leveling before further increase. This is another area where ongoing transmission events (i.e. school reopenings) could drive things further upward. We need more time to know.
This was the week, however, that deaths began to climb dramatically, rising by 146%. We can see that deaths are rising fastest for rural counties, which is consistent with previous surges. But death rate in the Atlanta suburbs is tracking at a similar pace compared to rural counties, just starting at a lower position. Death rate is rising more gradually for nonrural counties. For Atlanta counties (Fulton + DeKalb) the death rate looks like it’s still within the “noise” of week to week variation.

Let’s look at how the deaths were distributed this week across age groups. The biggest areas of increase were for age groups 50-80+. This week the state also recorded a new pediatric death - a 17 year old male from Douglas county.

But the vaccine has changed the distribution of deaths in this surge, so far. The graph above is for the most recent surge (just beginning). The graph below shows how the surge in deaths unfolded during the winter 2020-2021 surge.

In the past, we’ve seen that by a large margin the majority of deaths were in those 80+. Since this older population was aggressively targeted for vaccination, it’s a good thing to see that their weekly death count is on par with 60-69 year olds, so far at least. If this trend holds, it means that the deaths associated with the summer 2021 surge will have a younger age distribution than previous surges. It is a reminder of the success of the vaccine so far, but also the deficiencies of the vaccination effort because these deaths are preventable. We just didn’t get to them in time with a vaccine or they declined the vaccine when it was available to them.
Parenting an unvaccinated child during the delta surge
This week my family made decisions to cancel vacation travel and concert tickets that were purchased in March. We were riding the high of vaccinations and the freedom we expected to have with them, while also assuming that a pediatric vaccine would be available by fall. Instead, here we sit with a 10 year old who is too young to be vaccinated as cases surge in our area (Kansas City).
The vacation was scheduled for Labor Day weekend and would have featured air travel with multiple layovers. The concert was Garth Brooks. Even though it is an outdoor concert, I’m not taking any risks.
The news reports seem to waffle when it comes to when the Emergency Use Authorization will be granted for kids aged 11 and under. I read a report yesterday where Pfizer indicated they expected EUA by the end of September. However, I’m concerned that even this estimate, which is better than the “mid-winter” estimates we were given earlier, will be too late to protect the majority of America’s school-aged children. With the heightened transmission of the delta variant compared to previous variants and the lack of disease mitigation standards universally applied across all schools, I would not be surprised if virtually all US school children are exposed in the lunchroom or elsewhere in the building by the end of September.
References
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
https://www.salon.com/2021/08/02/under-12-covid-vaccine/
The COVID Digest is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology and I am Chair of the Division of Natural Sciences and Mathematics at the University of Saint Mary. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion, do not represent the views or opinions of my employer and should not be considered medical advice.