

The COVID Digest, 04May2021
Georgia COVID-19 Updates

Vaccine Update
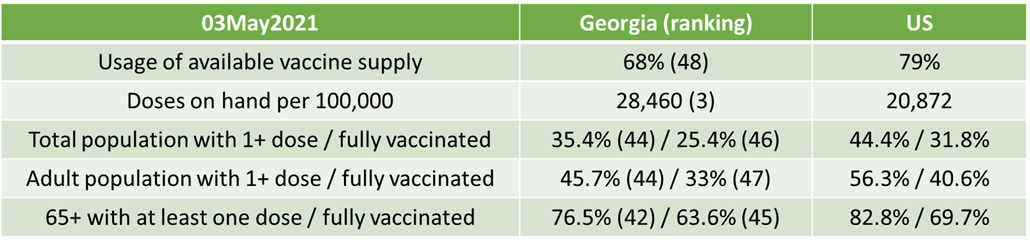
The data provided in the table below are publicly available from the CDC update as of the morning of 03May2021. The table compares Georgia’s data to the US average. CDC indicates that 9.48 million doses have been delivered in the state and 6.46 million have been administered in the state of Georgia. That leaves an inventory of 3,021,701 doses on hand. This week, the state moved up in the rankings for the 3rd largest stockpile of unused vaccines, 36% higher than the national average. The state moved up in the rankings by one position each for total and adult population that is fully vaccinated. The state is well off the national pace, however.
You may have heard two pieces of news on the vaccine front. First, Pfizer is expected to be granted expanded Emergency Use Authorization for 12-15 year olds this week. Second, Pfizer is allegedly planning to apply for full FDA approval (not emergency use authorization) of its COVID-19 vaccine this month. Full FDA approval will change the conversation when it comes to requiring vaccination as compared to encouraging vaccination for access to certain activities (i.e. military, colleges and workplaces). Or as a condition of holding certain positions, such as working in a long term care facility. Full approval may also help to win over some of the persuadable population who was waiting to see this process through to its regulatory finish line before taking the vaccine. For the EUA expansion to adolescents, this is a big step forward for a lot of parents concerned about summer camps and safe return to school in the fall. This is especially important for children from racial or ethnic minority populations who have been harmed disproportionately by COVID-19 disease than their White counterparts. The graph below shows deaths for K-12 aged children and how their proportion of COVID-19 deaths compares to their makeup of the total population, generated by the CDC. We can see that Hispanic/Latinx, Black, American Indian / Alaska Native and Multiple/Other populations are all outperforming on death due to COVID-19, relative to their proportion of the 5-17 year old population. The push to reopen schools has largely discarded this concern - that school in its current form may not be a safe environment for everyone there, especially if there is not a strong safety culture for COVID-19. With COVID-19 you share the risks that were taken by the people around you. If someone around you has been living their best life for the past year and assuming a lot of risk, that puts you at greater risk especially if you have been careful or have an underlying condition. I want kids back in school as much as possible (including my own!) but it will be safer for everyone involved and more like normal if we can make vaccines available to families. That way the risks that some force onto others can be mitigated.

Another great thing about vaccine eligibility extending down to 12 year olds and up is that America and Georgia already has good infrastructure to serve this population, their families and the surrounding community - public schools. Public schools have drive through routing for cars and busses. They have cafeterias, gymnasiums and hallways that can space people out for vaccinations, much like we do for voting. Hand out popsicles on the playground during the post-vaccine waiting period. With the coming heat of Georgia summer, this kind of infrastructure that exists in all 159 counties could be a very big deal. Last year, we also saw school busses that took meals neighborhood to neighborhood, knowing that food insecurity was going to be a big problem for many of their students. Can we team vaccinators up with that key piece of infrastructure to ensure children and families who wish to be vaccinated have service at their door? We already have some of the tools we need to be successful here. We need to match resources to needs and make things happen.
If you look at what’s happening in other countries, especially India, you can appreciate the question of why we’re considering vaccinating children at all right now, since on average they have less risk of severe complications than older adults. Should we prioritize vaccine shipments instead to other countries that are hot spots right now? I can understand and appreciate this sense of altruism. But we saw this before when doses were being thrown out at the end of the day because vaccine clinics couldn’t find enough senior citizens or healthcare workers. Personally, my feelings on it have to do with how the vaccines have been distributed to date. A vaccine in the freezer or in a trash can does no one any good. Use what is already distributed, share what hasn’t been distributed yet. Unless we are going to round up the 3 million doses in freezers across Georgia and ship them overseas, we need to vaccinate the closest willing human, even if they’re comparatively low risk (low does not equal zero risk anyway). With each person we vaccinate, that’s fewer transmission opportunities to vulnerable people that we haven’t been able to vaccinate yet or who refuse to be vaccinated entirely. I think we can and should release all of the AstraZeneca doses that the US has been stockpiling to other countries and perhaps prioritize future shipments of vaccine to other countries too. I think with 3 million doses on hand, Georgia could afford to take a week or two off if they had to do so. If we aren’t going to use this life saving technology, there are millions of people around the world right now who would do anything to have them. I hope many can appreciate how very fortunate they are to have been born in the time and place that these vaccines were available to us first. The privilege we have is not a luxury that was afforded to the rest of the world.
The United States

The map above comes from the CDC COVID-19 Tracker on the Community tab, county view. The map above looks at the combined community transmission indicators that looks at both case rate and test positivity. Red and orange are considered the danger zone, yellow is safer and blue is safest. Nationally, the areas of greatest intensity are the upper Midwest and Northeast, Pacific Northwest and Colorado. Closer to Georgia, many of its neighbors majority red/orange including Tennessee, the Carolinas and Florida.
The table below tells you where we are this week and how that compares to the previous week (in parentheses). The data for everything comes from the HHS Community Profile Report from 03May2021.

Georgia has just one county in the top 20 counties in the US for new case rate per 100,000 residents - Chattahoochee county at #12, down from #4 the previous week.
The table below shows the highest and lowest ranking states and territories from the latest HHS State Reports (formerly known as the White House Coronavirus Task Force Reports). You can find the most recent report here.

Certain states are in the top five for multiple non-vaccine metrics, including California, Hawaii, Arkansas and Mississippi. Then there are states like Michigan that are consistently ranked the worst or nearly the worst in the nation. Other states that make multiple appearances in the “worst” rankings are Pennsylvania, Florida and Delaware. Of note, even though Georgia’s death rate is lower than the pre-winter surge baseline, it is the highest death rate in the nation from COVID-19.
Georgia
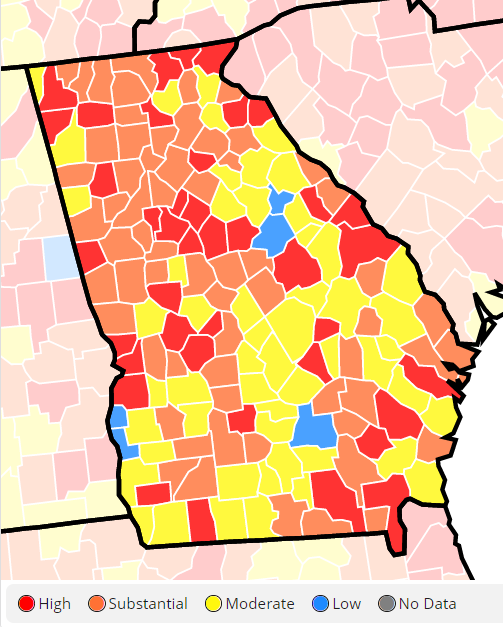
We can zoom in on a current view of Georgia using the CDC community transmission criteria. Last week, there were 4 counties in the blue category and 50 counties in the yellow category, with 66% of Georgia’s counties in the substantial or high transmission categories. This week, there are 5 blue counties and 49 counties in the yellow category. So there are still 66% of the state’s counties in the substantial or high transmission categories. Nationally, 68.5% of US counties are in the red or orange zone. So Georgia is performing slightly below the national average, in a good way.
This week, more of the Atlanta metro has shifted from red to orange, continuing the trend from the previous week. This is really good news since this is where Georgia’s population is most dense. Things are getting better along the southwestern border of the state with Alabama and Florida.
From the most recent HHS State Report (formerly known as the White House Coronavirus Task Force reports), the graph below shows how the proportion of Georgia counties in each color class has shifted over time. It’s been a bouncy trajectory, but the trend has been a decreasing proportion of counties in the red zone since mid-March and an expansion of yellow or blue counties. That progress seemed to go away this week with a growth in the red and orange county classes.

Testing
According to the most recent HHS Community Profile report, Georgia is ranked #35 in the nation for test positivity (yellow zone) and #46 in the nation for tests performed per 100,000 (with 1 best best for both), in the orange zone.
If we drill down to Georgia in the HHS data, we can see the following test positivity rate by age group in the chart below. Only children <5 and adults 65+ are under 5% test positivity. We are undercounting disease in all other age groups, and especially among K-12 aged children, 5-17.
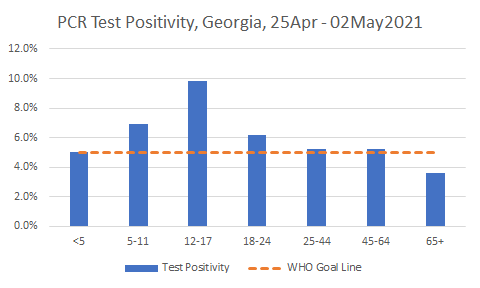
It was a low day for PCR testing volume day for Georgia but not for antigen testing. There were 9,802 newly reported PCR tests and 5.9% were positive. There were 11,221 newly reported antigen tests and 5.5% were positive.
Cases
Cases are flat for Georgia and decreasing for the nation. Georgia is ranked #24 (with 1 being best) for new case rate, in the orange zone, according to the 30Apr2021 HHS Community Profile Reports. So the state is right in the middle of the pack.
Today there was a net increase of 1178 newly reported cases for Georgia, with 690 identified by PCR and 488 by antigen testing. The state’s case rate is relatively flat, about 6.1% higher than the post-winter surge low point, set on 06Apr.
Hospitalizations
Today there were 94 newly reported COVID-19 hospital admissions and 11 admissions to the ICU. These are lower numbers than are typical for a Tuesday.
For confirmed COVID-19 hospital admissions per 100 beds, Georgia is ranked #35 in the country (with #1 being best), in the yellow zone.
I brought the next graph up on Sunday but want to reiterate an observation. The graph shows weekly hospitalization numbers for COVID-19 (confirmed by PCR prior to admission) for each age group. If you look at the dashed gray line between 50-59 and 60-69, what do you notice?

Things aren’t going up and down temporally, as they would during a surge…meaning that things more or less go up and down for different age groups together. To the left of the line, hospitalizations are trending up weekly. To the right of the line, hospitalizations are trending down. There were nearly as many 30-39 year olds hospitalized last week as there were 80+. There were more 40-49 year olds admitted than 70-79 year olds. I think the vaccine is responsible for both sides of the gray line but in different ways. On the right, vaccines are protecting older adults from the more severe forms of COVID-19 that require hospitalization - exactly what we want them to do. On the left, the knowledge that a vaccine is protecting older adults, growing pandemic fatigue and easing of pandemic restrictions might mean that younger adults are taking more risks. We need to do more to make vaccines available to younger adults and encourage people to take them. Then we might expect to see these trends flatten or trend downward for younger adults as well.
This doesn’t even touch what happens with Long COVID-19 among younger adults with a lot of life to live. Keep in mind, we don’t vaccinate people for polio because it kills a lot of people. We vaccinate against polio because of the life-altering paralysis that can result. We don’t vaccinate for chickenpox (Varicella) because it has a high mortality rate. We vaccinate because it can be life threatening for some, cause disfigurement in others, and because Shingles later in life is excruciating and should be avoided. So when young people ask me why they should be vaccinated one of my biggest reasons is because I don’t want the results of a preventable infection to change their life or limit what they can do in the future. I don’t want permanent cardiac damage to keep them from running a marathon, playing with their kids, or joining the military. I don’t want a preventable pre-existing condition for you that disqualifies you from life insurance. This isn’t influenza where people more or less return to their pre-infection state of health. There are people experiencing prolonged quality of life problems for as much as 8 months following recovery from infection, even in those who didn’t require a hospital stay for COVID-19. Young adults are awesome but not invincible. With our state and national slow down in vaccine uptake, COVID-19 is going to still be with us when younger adults age into older ones when their risk will rise with each passing decade. Why put off protecting yourself from something we can prevent, safely and effectively?
Deaths
Death rate is flat for the US and increasing just a bit for Georgia. Georgia is ranked #51 in the US (with 1 being best) for new death rate per 100,000, in the red zone, according to the 30Apr HHS State Profile Report.

Today Georgia reported a net increase of 11 newly reported confirmed COVID-19 deaths and 3 probable deaths. This is a low day, thank goodness. The state’s death rate per 100,000 is now 27% below the pre-winter surge baseline, a very good place to be. Let’s keep that going. Get vaccinated or help those around you to get vaccinated.
References
https://covid.cdc.gov/covid-data-tracker/#vaccinations
https://dph.georgia.gov/covid-19-daily-status-report
https://covid-gagio.hub.arcgis.com/
https://covid.cdc.gov/covid-data-tracker/#county-view
https://beta.healthdata.gov/Health/COVID-19-Community-Profile-Report/gqxm-d9w9
https://www.nytimes.com/live/2021/05/03/world/covid-vaccine-coronavirus-cases#pfizer-covid-vaccine-teens
https://www.cnbc.com/2021/05/04/pfizer-pfe-earnings-q1-2021.html
https://covid.cdc.gov/covid-data-tracker/#demographics
Georgia COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.